

The fascinating history of clinical trials

Professor of Biostatistics, University of South Australia
Disclosure statement
Adrian Esterman does not work for, consult, own shares in or receive funding from any company or organisation that would benefit from this article, and has disclosed no relevant affiliations beyond their academic appointment.
University of South Australia provides funding as a member of The Conversation AU.
View all partners
Clinical trials are under way around the world, including in Australia, testing COVID-19 vaccines and treatments .
These clinical trials largely fall into two groups. With observational studies , researchers follow a group of people to see what happens to them. With experimental studies , people are assigned to treatments, then followed.
These study designs have come about from centuries of people trying out different ways of treating people.
Here are some of the key moments in the history of clinical trials that led to the type of trials we see today for COVID-19.
Read more: From the research lab to your doctor's office – here's what happens in phase 1, 2, 3 drug trials
Ginseng in 11th-century China
One of the earliest observational studies occurred nearly 1,000 years ago in China. The 1061 Atlas of Materia Medica (Ben Cao Tu Jing) was compiled and edited by Song Su , a renowned scientist, administrator, diplomat and military strategist.
It documented a trial of ginseng:
[…] to evaluate the effect of genuine Shangdang ginseng, two persons were asked to run together. One was given the ginseng while the other ran without. After running for approximately three to five li [about 1,500-2,500 metres], the one without the ginseng developed severe shortness of breath, while the one who took the ginseng breathed evenly and smoothly.
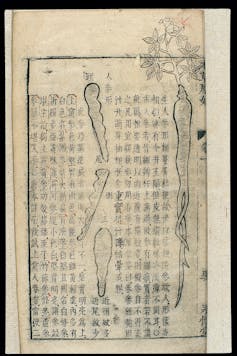
This observational study is also the first recorded example of a control group .
A control group can be patients who are not treated at all, patients who receive a standard treatment compared to a new one, or patients who receive a placebo (a treatment or substance designed to have no therapeutic effect).
Having a control group is one of the cornerstones of modern clinical trials.
An example of a control group in COVID-19 research is this recent study . People with diabetes hospitalised for COVID-19 were divided into those receiving the drug metformin and those not receiving it (the control group).
Back to ginseng. Today, it is a popular herbal remedy. As to whether it improves stamina, a recent review found some evidence ginseng might help men with erectile dysfunction .
Rhubarb in 18th-century England

Rhubarb roots have been used as a laxative for more than 5,000 years , including in 18th-century England.
Caleb Parry , an English physician working in Bath, wanted to know whether locally grown rhubarb was as good as the more expensive Turkish variety.
In 1786, he ran a study in which he switched the type of rhubarb he gave to each patient at different times. He then compared each patient’s symptoms while eating each type of rhubarb. He concluded there was no advantage in using the Turkish version.
This is the first published example of a crossover trial (a study where the participants receive each treatment at different times).
Today, we know rhubarb roots and stems are rich in anthraquinones , which have a laxative effect .
Early 20th-century randomised trial
Beriberi , a disease that can have lasting effects on the nervous system and heart, was common in Southeast Asia in the early part of the 20th century.
In 1905 a beriberi outbreak occured at the Kuala Lumpur Lunatic Asylum. At that time William Fletcher was the district surgeon. He realised the outbreak provided an excellent opportunity to run an experiment (which we now know is just a bit unethical).
Read more: Looking back on the chequered past of drug trials
Each patient was assigned a number. Those with even numbers were sent to one ward and given brown unpolished rice to eat. Those with odd numbers went to another ward and given white polished rice.
At the end of the experiment, 15% of the patients who ate the white rice died of beriberi; none given brown rice died.
Read more: Health Check: can vitamins supplement a poor diet?
This is a very early example of randomisation in a clinical trial, where one group is chosen at random to receive a treatment.
Randomisation is another very important factor in good clinical trial design.
Today we know beriberi is caused by a deficiency in thiamine (vitamin B1) and a white rice diet is deficient in thiamine .
Tuberculosis and the randomised controlled trial

Sir Austin Bradford Hill , an English epidemiologist and statistician, conducted the first randomised controlled trial in 1948. The trial was to treat the lung disease tuberculosis.
Bradford Hill decided whether a patient should be treated with the antibiotic streptomycin plus bed rest, or bed rest alone, by using a table of random numbers.
The investigators didn’t know which patient got each treatment; details were in sealed envelopes. Patients were not told they were in a trial.
Using sealed envelopes is an example of what we now call allocation concealment . Making sure neither investigators nor patients know which treatment they are receiving is called blinding . These are now standard features of randomised controlled trials.
Randomised controlled trials are the “gold standard” of clinical trial designs, due to the use of both a control group and randomisation.
Decades later, researchers have used a randomised controlled trial to test the drug ruxolitinib in patients with severe COVID-19.
So, although Bradford Hill conducted the first randomised controlled trial, it was based on hundreds of years of people working out why things like a control group and randomisation are so important.
Read more: Randomised control trials: what makes them the gold standard in medical research?
- Pharmaceuticals
- Clinical trials
- Coronavirus
- History of science
- History of medicine
- Vaccine trials
Faculty of Law - Academic Appointment Opportunities
Operations Manager
Senior Education Technologist
Audience Development Coordinator (fixed-term maternity cover)
Lecturer (Hindi-Urdu)
- Search Menu
- Browse content in Arts and Humanities
- Browse content in Archaeology
- Anglo-Saxon and Medieval Archaeology
- Archaeological Methodology and Techniques
- Archaeology by Region
- Archaeology of Religion
- Archaeology of Trade and Exchange
- Biblical Archaeology
- Contemporary and Public Archaeology
- Environmental Archaeology
- Historical Archaeology
- History and Theory of Archaeology
- Industrial Archaeology
- Landscape Archaeology
- Mortuary Archaeology
- Prehistoric Archaeology
- Underwater Archaeology
- Urban Archaeology
- Zooarchaeology
- Browse content in Architecture
- Architectural Structure and Design
- History of Architecture
- Residential and Domestic Buildings
- Theory of Architecture
- Browse content in Art
- Art Subjects and Themes
- History of Art
- Industrial and Commercial Art
- Theory of Art
- Biographical Studies
- Byzantine Studies
- Browse content in Classical Studies
- Classical History
- Classical Philosophy
- Classical Mythology
- Classical Literature
- Classical Reception
- Classical Art and Architecture
- Classical Oratory and Rhetoric
- Greek and Roman Epigraphy
- Greek and Roman Law
- Greek and Roman Archaeology
- Greek and Roman Papyrology
- Late Antiquity
- Religion in the Ancient World
- Digital Humanities
- Browse content in History
- Colonialism and Imperialism
- Diplomatic History
- Environmental History
- Genealogy, Heraldry, Names, and Honours
- Genocide and Ethnic Cleansing
- Historical Geography
- History by Period
- History of Agriculture
- History of Education
- History of Emotions
- History of Gender and Sexuality
- Industrial History
- Intellectual History
- International History
- Labour History
- Legal and Constitutional History
- Local and Family History
- Maritime History
- Military History
- National Liberation and Post-Colonialism
- Oral History
- Political History
- Public History
- Regional and National History
- Revolutions and Rebellions
- Slavery and Abolition of Slavery
- Social and Cultural History
- Theory, Methods, and Historiography
- Urban History
- World History
- Browse content in Language Teaching and Learning
- Language Learning (Specific Skills)
- Language Teaching Theory and Methods
- Browse content in Linguistics
- Applied Linguistics
- Cognitive Linguistics
- Computational Linguistics
- Forensic Linguistics
- Grammar, Syntax and Morphology
- Historical and Diachronic Linguistics
- History of English
- Language Acquisition
- Language Variation
- Language Families
- Language Evolution
- Language Reference
- Lexicography
- Linguistic Theories
- Linguistic Typology
- Linguistic Anthropology
- Phonetics and Phonology
- Psycholinguistics
- Sociolinguistics
- Translation and Interpretation
- Writing Systems
- Browse content in Literature
- Bibliography
- Children's Literature Studies
- Literary Studies (Asian)
- Literary Studies (European)
- Literary Studies (Eco-criticism)
- Literary Studies (Modernism)
- Literary Studies (Romanticism)
- Literary Studies (American)
- Literary Studies - World
- Literary Studies (1500 to 1800)
- Literary Studies (19th Century)
- Literary Studies (20th Century onwards)
- Literary Studies (African American Literature)
- Literary Studies (British and Irish)
- Literary Studies (Early and Medieval)
- Literary Studies (Fiction, Novelists, and Prose Writers)
- Literary Studies (Gender Studies)
- Literary Studies (Graphic Novels)
- Literary Studies (History of the Book)
- Literary Studies (Plays and Playwrights)
- Literary Studies (Poetry and Poets)
- Literary Studies (Postcolonial Literature)
- Literary Studies (Queer Studies)
- Literary Studies (Science Fiction)
- Literary Studies (Travel Literature)
- Literary Studies (War Literature)
- Literary Studies (Women's Writing)
- Literary Theory and Cultural Studies
- Mythology and Folklore
- Shakespeare Studies and Criticism
- Browse content in Media Studies
- Browse content in Music
- Applied Music
- Dance and Music
- Ethics in Music
- Ethnomusicology
- Gender and Sexuality in Music
- Medicine and Music
- Music Cultures
- Music and Religion
- Music and Culture
- Music and Media
- Music Education and Pedagogy
- Music Theory and Analysis
- Musical Scores, Lyrics, and Libretti
- Musical Structures, Styles, and Techniques
- Musicology and Music History
- Performance Practice and Studies
- Race and Ethnicity in Music
- Sound Studies
- Browse content in Performing Arts
- Browse content in Philosophy
- Aesthetics and Philosophy of Art
- Epistemology
- Feminist Philosophy
- History of Western Philosophy
- Metaphysics
- Moral Philosophy
- Non-Western Philosophy
- Philosophy of Science
- Philosophy of Action
- Philosophy of Law
- Philosophy of Religion
- Philosophy of Language
- Philosophy of Mind
- Philosophy of Perception
- Philosophy of Mathematics and Logic
- Practical Ethics
- Social and Political Philosophy
- Browse content in Religion
- Biblical Studies
- Christianity
- East Asian Religions
- History of Religion
- Judaism and Jewish Studies
- Qumran Studies
- Religion and Education
- Religion and Health
- Religion and Politics
- Religion and Science
- Religion and Law
- Religion and Art, Literature, and Music
- Religious Studies
- Browse content in Society and Culture
- Cookery, Food, and Drink
- Cultural Studies
- Customs and Traditions
- Ethical Issues and Debates
- Hobbies, Games, Arts and Crafts
- Lifestyle, Home, and Garden
- Natural world, Country Life, and Pets
- Popular Beliefs and Controversial Knowledge
- Sports and Outdoor Recreation
- Technology and Society
- Travel and Holiday
- Visual Culture
- Browse content in Law
- Arbitration
- Browse content in Company and Commercial Law
- Commercial Law
- Company Law
- Browse content in Comparative Law
- Systems of Law
- Competition Law
- Browse content in Constitutional and Administrative Law
- Government Powers
- Judicial Review
- Local Government Law
- Military and Defence Law
- Parliamentary and Legislative Practice
- Construction Law
- Contract Law
- Browse content in Criminal Law
- Criminal Procedure
- Criminal Evidence Law
- Sentencing and Punishment
- Employment and Labour Law
- Environment and Energy Law
- Browse content in Financial Law
- Banking Law
- Insolvency Law
- History of Law
- Human Rights and Immigration
- Intellectual Property Law
- Browse content in International Law
- Private International Law and Conflict of Laws
- Public International Law
- IT and Communications Law
- Jurisprudence and Philosophy of Law
- Law and Politics
- Law and Society
- Browse content in Legal System and Practice
- Courts and Procedure
- Legal Skills and Practice
- Primary Sources of Law
- Regulation of Legal Profession
- Medical and Healthcare Law
- Browse content in Policing
- Criminal Investigation and Detection
- Police and Security Services
- Police Procedure and Law
- Police Regional Planning
- Browse content in Property Law
- Personal Property Law
- Study and Revision
- Terrorism and National Security Law
- Browse content in Trusts Law
- Wills and Probate or Succession
- Browse content in Medicine and Health
- Browse content in Allied Health Professions
- Arts Therapies
- Clinical Science
- Dietetics and Nutrition
- Occupational Therapy
- Operating Department Practice
- Physiotherapy
- Radiography
- Speech and Language Therapy
- Browse content in Anaesthetics
- General Anaesthesia
- Neuroanaesthesia
- Browse content in Clinical Medicine
- Acute Medicine
- Cardiovascular Medicine
- Clinical Genetics
- Clinical Pharmacology and Therapeutics
- Dermatology
- Endocrinology and Diabetes
- Gastroenterology
- Genito-urinary Medicine
- Geriatric Medicine
- Infectious Diseases
- Medical Oncology
- Medical Toxicology
- Pain Medicine
- Palliative Medicine
- Rehabilitation Medicine
- Respiratory Medicine and Pulmonology
- Rheumatology
- Sleep Medicine
- Sports and Exercise Medicine
- Clinical Neuroscience
- Community Medical Services
- Critical Care
- Emergency Medicine
- Forensic Medicine
- Haematology
- History of Medicine
- Browse content in Medical Dentistry
- Oral and Maxillofacial Surgery
- Paediatric Dentistry
- Restorative Dentistry and Orthodontics
- Surgical Dentistry
- Medical Ethics
- Browse content in Medical Skills
- Clinical Skills
- Communication Skills
- Nursing Skills
- Surgical Skills
- Medical Statistics and Methodology
- Browse content in Neurology
- Clinical Neurophysiology
- Neuropathology
- Nursing Studies
- Browse content in Obstetrics and Gynaecology
- Gynaecology
- Occupational Medicine
- Ophthalmology
- Otolaryngology (ENT)
- Browse content in Paediatrics
- Neonatology
- Browse content in Pathology
- Chemical Pathology
- Clinical Cytogenetics and Molecular Genetics
- Histopathology
- Medical Microbiology and Virology
- Patient Education and Information
- Browse content in Pharmacology
- Psychopharmacology
- Browse content in Popular Health
- Caring for Others
- Complementary and Alternative Medicine
- Self-help and Personal Development
- Browse content in Preclinical Medicine
- Cell Biology
- Molecular Biology and Genetics
- Reproduction, Growth and Development
- Primary Care
- Professional Development in Medicine
- Browse content in Psychiatry
- Addiction Medicine
- Child and Adolescent Psychiatry
- Forensic Psychiatry
- Learning Disabilities
- Old Age Psychiatry
- Psychotherapy
- Browse content in Public Health and Epidemiology
- Epidemiology
- Public Health
- Browse content in Radiology
- Clinical Radiology
- Interventional Radiology
- Nuclear Medicine
- Radiation Oncology
- Reproductive Medicine
- Browse content in Surgery
- Cardiothoracic Surgery
- Gastro-intestinal and Colorectal Surgery
- General Surgery
- Neurosurgery
- Paediatric Surgery
- Peri-operative Care
- Plastic and Reconstructive Surgery
- Surgical Oncology
- Transplant Surgery
- Trauma and Orthopaedic Surgery
- Vascular Surgery
- Browse content in Science and Mathematics
- Browse content in Biological Sciences
- Aquatic Biology
- Biochemistry
- Bioinformatics and Computational Biology
- Developmental Biology
- Ecology and Conservation
- Evolutionary Biology
- Genetics and Genomics
- Microbiology
- Molecular and Cell Biology
- Natural History
- Plant Sciences and Forestry
- Research Methods in Life Sciences
- Structural Biology
- Systems Biology
- Zoology and Animal Sciences
- Browse content in Chemistry
- Analytical Chemistry
- Computational Chemistry
- Crystallography
- Environmental Chemistry
- Industrial Chemistry
- Inorganic Chemistry
- Materials Chemistry
- Medicinal Chemistry
- Mineralogy and Gems
- Organic Chemistry
- Physical Chemistry
- Polymer Chemistry
- Study and Communication Skills in Chemistry
- Theoretical Chemistry
- Browse content in Computer Science
- Artificial Intelligence
- Computer Architecture and Logic Design
- Game Studies
- Human-Computer Interaction
- Mathematical Theory of Computation
- Programming Languages
- Software Engineering
- Systems Analysis and Design
- Virtual Reality
- Browse content in Computing
- Business Applications
- Computer Security
- Computer Games
- Computer Networking and Communications
- Digital Lifestyle
- Graphical and Digital Media Applications
- Operating Systems
- Browse content in Earth Sciences and Geography
- Atmospheric Sciences
- Environmental Geography
- Geology and the Lithosphere
- Maps and Map-making
- Meteorology and Climatology
- Oceanography and Hydrology
- Palaeontology
- Physical Geography and Topography
- Regional Geography
- Soil Science
- Urban Geography
- Browse content in Engineering and Technology
- Agriculture and Farming
- Biological Engineering
- Civil Engineering, Surveying, and Building
- Electronics and Communications Engineering
- Energy Technology
- Engineering (General)
- Environmental Science, Engineering, and Technology
- History of Engineering and Technology
- Mechanical Engineering and Materials
- Technology of Industrial Chemistry
- Transport Technology and Trades
- Browse content in Environmental Science
- Applied Ecology (Environmental Science)
- Conservation of the Environment (Environmental Science)
- Environmental Sustainability
- Environmentalist Thought and Ideology (Environmental Science)
- Management of Land and Natural Resources (Environmental Science)
- Natural Disasters (Environmental Science)
- Nuclear Issues (Environmental Science)
- Pollution and Threats to the Environment (Environmental Science)
- Social Impact of Environmental Issues (Environmental Science)
- History of Science and Technology
- Browse content in Materials Science
- Ceramics and Glasses
- Composite Materials
- Metals, Alloying, and Corrosion
- Nanotechnology
- Browse content in Mathematics
- Applied Mathematics
- Biomathematics and Statistics
- History of Mathematics
- Mathematical Education
- Mathematical Finance
- Mathematical Analysis
- Numerical and Computational Mathematics
- Probability and Statistics
- Pure Mathematics
- Browse content in Neuroscience
- Cognition and Behavioural Neuroscience
- Development of the Nervous System
- Disorders of the Nervous System
- History of Neuroscience
- Invertebrate Neurobiology
- Molecular and Cellular Systems
- Neuroendocrinology and Autonomic Nervous System
- Neuroscientific Techniques
- Sensory and Motor Systems
- Browse content in Physics
- Astronomy and Astrophysics
- Atomic, Molecular, and Optical Physics
- Biological and Medical Physics
- Classical Mechanics
- Computational Physics
- Condensed Matter Physics
- Electromagnetism, Optics, and Acoustics
- History of Physics
- Mathematical and Statistical Physics
- Measurement Science
- Nuclear Physics
- Particles and Fields
- Plasma Physics
- Quantum Physics
- Relativity and Gravitation
- Semiconductor and Mesoscopic Physics
- Browse content in Psychology
- Affective Sciences
- Clinical Psychology
- Cognitive Neuroscience
- Cognitive Psychology
- Criminal and Forensic Psychology
- Developmental Psychology
- Educational Psychology
- Evolutionary Psychology
- Health Psychology
- History and Systems in Psychology
- Music Psychology
- Neuropsychology
- Organizational Psychology
- Psychological Assessment and Testing
- Psychology of Human-Technology Interaction
- Psychology Professional Development and Training
- Research Methods in Psychology
- Social Psychology
- Browse content in Social Sciences
- Browse content in Anthropology
- Anthropology of Religion
- Human Evolution
- Medical Anthropology
- Physical Anthropology
- Regional Anthropology
- Social and Cultural Anthropology
- Theory and Practice of Anthropology
- Browse content in Business and Management
- Business Strategy
- Business History
- Business Ethics
- Business and Government
- Business and Technology
- Business and the Environment
- Comparative Management
- Corporate Governance
- Corporate Social Responsibility
- Entrepreneurship
- Health Management
- Human Resource Management
- Industrial and Employment Relations
- Industry Studies
- Information and Communication Technologies
- International Business
- Knowledge Management
- Management and Management Techniques
- Operations Management
- Organizational Theory and Behaviour
- Pensions and Pension Management
- Public and Nonprofit Management
- Strategic Management
- Supply Chain Management
- Browse content in Criminology and Criminal Justice
- Criminal Justice
- Criminology
- Forms of Crime
- International and Comparative Criminology
- Youth Violence and Juvenile Justice
- Development Studies
- Browse content in Economics
- Agricultural, Environmental, and Natural Resource Economics
- Asian Economics
- Behavioural Finance
- Behavioural Economics and Neuroeconomics
- Econometrics and Mathematical Economics
- Economic Systems
- Economic Methodology
- Economic History
- Economic Development and Growth
- Financial Markets
- Financial Institutions and Services
- General Economics and Teaching
- Health, Education, and Welfare
- History of Economic Thought
- International Economics
- Labour and Demographic Economics
- Law and Economics
- Macroeconomics and Monetary Economics
- Microeconomics
- Public Economics
- Urban, Rural, and Regional Economics
- Welfare Economics
- Browse content in Education
- Adult Education and Continuous Learning
- Care and Counselling of Students
- Early Childhood and Elementary Education
- Educational Equipment and Technology
- Educational Strategies and Policy
- Higher and Further Education
- Organization and Management of Education
- Philosophy and Theory of Education
- Schools Studies
- Secondary Education
- Teaching of a Specific Subject
- Teaching of Specific Groups and Special Educational Needs
- Teaching Skills and Techniques
- Browse content in Environment
- Applied Ecology (Social Science)
- Climate Change
- Conservation of the Environment (Social Science)
- Environmentalist Thought and Ideology (Social Science)
- Natural Disasters (Environment)
- Social Impact of Environmental Issues (Social Science)
- Browse content in Human Geography
- Cultural Geography
- Economic Geography
- Political Geography
- Browse content in Interdisciplinary Studies
- Communication Studies
- Museums, Libraries, and Information Sciences
- Browse content in Politics
- African Politics
- Asian Politics
- Chinese Politics
- Comparative Politics
- Conflict Politics
- Elections and Electoral Studies
- Environmental Politics
- European Union
- Foreign Policy
- Gender and Politics
- Human Rights and Politics
- Indian Politics
- International Relations
- International Organization (Politics)
- International Political Economy
- Irish Politics
- Latin American Politics
- Middle Eastern Politics
- Political Methodology
- Political Communication
- Political Philosophy
- Political Sociology
- Political Theory
- Political Behaviour
- Political Economy
- Political Institutions
- Politics and Law
- Public Administration
- Public Policy
- Quantitative Political Methodology
- Regional Political Studies
- Russian Politics
- Security Studies
- State and Local Government
- UK Politics
- US Politics
- Browse content in Regional and Area Studies
- African Studies
- Asian Studies
- East Asian Studies
- Japanese Studies
- Latin American Studies
- Middle Eastern Studies
- Native American Studies
- Scottish Studies
- Browse content in Research and Information
- Research Methods
- Browse content in Social Work
- Addictions and Substance Misuse
- Adoption and Fostering
- Care of the Elderly
- Child and Adolescent Social Work
- Couple and Family Social Work
- Developmental and Physical Disabilities Social Work
- Direct Practice and Clinical Social Work
- Emergency Services
- Human Behaviour and the Social Environment
- International and Global Issues in Social Work
- Mental and Behavioural Health
- Social Justice and Human Rights
- Social Policy and Advocacy
- Social Work and Crime and Justice
- Social Work Macro Practice
- Social Work Practice Settings
- Social Work Research and Evidence-based Practice
- Welfare and Benefit Systems
- Browse content in Sociology
- Childhood Studies
- Community Development
- Comparative and Historical Sociology
- Economic Sociology
- Gender and Sexuality
- Gerontology and Ageing
- Health, Illness, and Medicine
- Marriage and the Family
- Migration Studies
- Occupations, Professions, and Work
- Organizations
- Population and Demography
- Race and Ethnicity
- Social Theory
- Social Movements and Social Change
- Social Research and Statistics
- Social Stratification, Inequality, and Mobility
- Sociology of Religion
- Sociology of Education
- Sport and Leisure
- Urban and Rural Studies
- Browse content in Warfare and Defence
- Defence Strategy, Planning, and Research
- Land Forces and Warfare
- Military Administration
- Military Life and Institutions
- Naval Forces and Warfare
- Other Warfare and Defence Issues
- Peace Studies and Conflict Resolution
- Weapons and Equipment

The Oxford Handbook of the History of Medicine
Mark Jackson is Professor of the History of Medicine at the University of Exeter and was Director of the Centre for Medical History there between 2000 and 2010. He served as Chair of the Wellcome Trust History of Medicine Funding Committee between 2003 and 2008 and is currently Chair of the Wellcome Trust Research Resources in Medical History Funding Committee. He has taught modules in the history of medicine and the history and philosophy of science for over twenty years at undergraduate and postgraduate levels to both medical and history students, and has also been involved in teaching medical history to GCSE and A-level students. His books include Newborn Child Murder (1996), The Borderland of Imbecility (2000), Infanticide: Historical Perspectives on Child Murder and Concealment 1550–2000 (ed., 2002), Allergy: The History of a Modern Malady (2006), Health and the Modern Home (ed., 2007), and Asthma: The Biography (2009). The Age of Stress: Science and the Search for Stability is due to be published by Oxford University Press in 2012.
- Cite Icon Cite
- Permissions Icon Permissions
The Oxford Handbook of the History of Medicine celebrates the richness and variety of medical history around the world. In recent decades, the history of medicine has emerged as a rich and mature sub-discipline within history, but the strength of the field has not precluded vigorous debates about methods, themes, and sources. Bringing together over thirty international scholars, this book provides a constructive overview of the current state of these debates, and offers new directions for future scholarship. There are three sections: the first explores the methodological challenges and historiographical debates generated by working in particular historical ages; the second explores the history of medicine in specific regions of the world and their medical traditions, and includes discussion of the ‘global history of medicine’; the final section analyses, from broad chronological and geographical perspectives, both established and emerging historical themes and methodological debates in the history of medicine.
Signed in as
Institutional accounts.
- Google Scholar Indexing
- GoogleCrawler [DO NOT DELETE]
Personal account
- Sign in with email/username & password
- Get email alerts
- Save searches
- Purchase content
- Activate your purchase/trial code
Institutional access
- Sign in with a library card Sign in with username/password Recommend to your librarian
- Institutional account management
- Get help with access
Access to content on Oxford Academic is often provided through institutional subscriptions and purchases. If you are a member of an institution with an active account, you may be able to access content in one of the following ways:
IP based access
Typically, access is provided across an institutional network to a range of IP addresses. This authentication occurs automatically, and it is not possible to sign out of an IP authenticated account.
Sign in through your institution
Choose this option to get remote access when outside your institution. Shibboleth/Open Athens technology is used to provide single sign-on between your institution’s website and Oxford Academic.
- Click Sign in through your institution.
- Select your institution from the list provided, which will take you to your institution's website to sign in.
- When on the institution site, please use the credentials provided by your institution. Do not use an Oxford Academic personal account.
- Following successful sign in, you will be returned to Oxford Academic.
If your institution is not listed or you cannot sign in to your institution’s website, please contact your librarian or administrator.
Sign in with a library card
Enter your library card number to sign in. If you cannot sign in, please contact your librarian.
Society Members
Society member access to a journal is achieved in one of the following ways:
Sign in through society site
Many societies offer single sign-on between the society website and Oxford Academic. If you see ‘Sign in through society site’ in the sign in pane within a journal:
- Click Sign in through society site.
- When on the society site, please use the credentials provided by that society. Do not use an Oxford Academic personal account.
If you do not have a society account or have forgotten your username or password, please contact your society.
Sign in using a personal account
Some societies use Oxford Academic personal accounts to provide access to their members. See below.
A personal account can be used to get email alerts, save searches, purchase content, and activate subscriptions.
Some societies use Oxford Academic personal accounts to provide access to their members.
Viewing your signed in accounts
Click the account icon in the top right to:
- View your signed in personal account and access account management features.
- View the institutional accounts that are providing access.
Signed in but can't access content
Oxford Academic is home to a wide variety of products. The institutional subscription may not cover the content that you are trying to access. If you believe you should have access to that content, please contact your librarian.
For librarians and administrators, your personal account also provides access to institutional account management. Here you will find options to view and activate subscriptions, manage institutional settings and access options, access usage statistics, and more.
Our books are available by subscription or purchase to libraries and institutions.
- About Oxford Academic
- Publish journals with us
- University press partners
- What we publish
- New features
- Open access
- Rights and permissions
- Accessibility
- Advertising
- Media enquiries
- Oxford University Press
- Oxford Languages
- University of Oxford
Oxford University Press is a department of the University of Oxford. It furthers the University's objective of excellence in research, scholarship, and education by publishing worldwide
- Copyright © 2024 Oxford University Press
- Cookie settings
- Cookie policy
- Privacy policy
- Legal notice
This Feature Is Available To Subscribers Only
Sign In or Create an Account
This PDF is available to Subscribers Only
For full access to this pdf, sign in to an existing account, or purchase an annual subscription.
Evolution of clinical research: a history before and beyond james lind
Affiliation.
- 1 President, Clininvent Research Pvt Ltd, Mumbai, India.
- PMID: 21829774
- PMCID: PMC3149409
The evolution of clinical research traverses a long and fascinating journey. From the first recorded trial of legumes in biblical times to the first randomized controlled of trial of streptomycin in 1946, the history of clinical trial covers a wide variety of challenges - scientific, ethical and regulatory. The famous 1747 scurvy trial conducted by James Lind contained most elements of a controlled trial. The UK Medical Research Council's (MRC) trial of patulin for common cold in 1943 was the first double blind controlled trial. This paved the way for the first randomized control trial of streptomycin in pulmonary tuberculosis carried out in 1946 by MRC of the UK. This landmark trial was a model of meticulousness in design and implementation, with systematic enrolment criteria and data collection compared with the ad hoc nature of other contemporary research. Over the years, as the discipline of controlled trials grew in sophistication and influence, the streptomycin trial continues to be referred to as ground breaking. The ethical advances in human protection include several milestones - Nuremberg Code, Declaration of Helsinki, Belmont Report, and 1996, International Conference on Harmonization Good Clinical Practice guidance. In parallel to ethical guidelines, clinical trials started to become embodied in regulation as government authorities began recognizing a need for controlling medical therapies in the early 20th century. As the scientific advances continue to occur, there will be new ethical and regulatory challenges requiring dynamic updates in ethical and legal framework of clinical trials.
Keywords: Clinical Trial; GCP; History; James Lind; Randomization.

Research Tools
Explore the historical collections.
Not sure which tool to use? Try the Research Tool Filter
Research Tool Filter
Show me tools that will help me find...
- Bibliographic References
- Datasets and APIs
- Digitized Collection Items
- Early Manuscripts
- Educational Resources
- Full Text Journal Articles
- Images to Download
- Institutional Archives
- Journal Articles back to the 17th Century
- Moving Pictures
- Personal Papers
- Public Domain Resources
- Topics in Medicine
- Uncataloged Materials
- Web Archives
LocatorPlus Catalog

Go To LocatorPlus Catalog
NLM’s holdings catalog for records for books, audiovisuals, journals, computer files, and other materials in the collections.
NLM Digital Collections

NLM’s free online resource of digitized biomedical books, still images, and videos available for viewing and download.
IndexCat™

NLM's signature database of medical bibliographic citations in the history of medicine.
Databases, Resources & APIs

Find, Use, and Reuse Data at NLM
PubMed Central

Full Text Journal Literature
Finding Aids

Archives, Manuscripts, Images, and Films
Images from the History of Medicine

Available in NLM Digital Collections.
NLM PROVIDES TWO CATALOG INTERFACES

LocatorPlus Catalog is the interface provided for onsite patrons in the Library’s reading room. It contains information on NLM holdings and circulation status, and provides access to the records in MARC format . Quick limits for searching historical collections and material formats are available. For help with searching LocatorPlus Catalog see NLM LocatorPlus Catalog Help .
Go to LOCATORPLUS CATALOG

NLM Catalog
The NLM Catalog provides access to NLM bibliographic data for over 1.4 million journals, books, audiovisuals, computer software, electronic resources, and other materials. It contains detailed MEDLINE indexing information about the journals in PubMed and other NCBI databases. Links to the library’s holdings in LocatorPlus Catalog are also provided. For help with searching the NLM Catalog see NLM Catalog Help .
Go to NLM Catalog
Journal citations.

PubMed comprises more than 26 million citations for biomedical literature from MEDLINE , life science journals, and online books. Citations may include links to full-text content from PubMed Central and publisher web sites. To find journal articles in the history of medicine, select “ Topic Specific-Queries ” from the “PubMed Tools” list on the PubMed homepage and select History of Medicine from the “Subjects” list. Full text of historically significant articles can be found in PubMed Central. For further information about PubMed, see NLM Customer Support .
Go to PUBMED
Full text articles.
")
PubMed Central® (PMC)
PubMed Central® (PMC) is a free full-text archive of biomedical and life sciences journal literature at the U.S. National Institutes of Health’s National Library of Medicine (NIH/NLM). PMC includes a growing collection of backfiles reaching back over two centuries.
AUDIOVISUAL COLLECTION GUIDES

Guide to Tropical Disease Motion Pictures and Audiovisuals
The Tropical Disease Motion Picture and Audiovisual Collection is comprised of films, videorecordings, and digital videocasts produced from the 1920s through 2009, with the majority shot prior to the 1960s. All are devoted to health concerns and include material on medicine and public health. Materials range from ideological, documentary, educational, and training films to American war propaganda. The intended audience is diverse and includes military personnel, health professionals, and the general public. The collection will be of particular interest to scholars concerned with the social, economic, and political implications of health disparities in a world where epidemics travel with great rapidity across national and regional borders.

Guide to Mental Health Motion Pictures
references to nearly 200 films and videorecordings produced from the 1930s up to and including 1970. Most deal with mental or psychiatric disorders as defined or recognized at the time the films were produced, as well as their corresponding causes and treatments. Some films focus on improving mental attitudes and thus overall health.
MODERN MANUSCRIPT COLLECTION GUIDES

Guide to Library and Archival Collections of African Americans in Medicine and Biomedical Research
The collections in this Guide are to assist in identifying useful medical history collections for researchers and scholars interested in African Americans in Medicine and Biomedical Research. Read More

History of Health Services Research Project
The project is motivated by the desire to collect the stories and experiences of innovators and leaders in the field of health services research. Read More

Medical Informatics Archival Collections
Medical informatics and medical librarianship form a strong collecting focus of the National Library of Medicine. Significant archival holdings on these topics are found within NLM’s institutional archives , and especially within the records of the Office of the Director, the Bibliographic Services Division (MEDLARS), and the Lister Hill Center. Many of NLM’s manuscripts collections are concerned with medical informatics, including the papers of NLM director John Shaw Billings, select personal and organizational archives, and the records and oral histories of the Medical Library Association (MLA).
ORAL HISTORY PROJECTS

Online Oral Histories
NLM has digitized selected material from its oral history collections. Content is organized into seven collections and includes digitized transcripts plus any accompanying audio content when available. Users can browse content by title, interviewee name, and subject. Full-text searching is available across all sub-collections, within each sub-collection, and within individual transcripts.
Search All Online Oral Histories
Go to project page.

This project is motivated by the desire to collect the stories and experiences of innovators and leaders in the field of health services research. It is co-sponsored by the National Information Center on Health Services Research and Health Care Technology (NICHSR) and the History of Medicine Division (HMD). Several initiatives are being pursued: individual oral and video interviews, a historical video for use in training health science librarians and HSR students, and solicitation and archiving of pertinent collections of papers.

Conversations with Medical Informatics Pioneers
Beginning in 2004, Drs. Joan S. Ash and Dean F. Sittig chose and interviewed seventeen medical informatics pioneers to capture their memories. In 2013, NLM acquired the transcripts from the first 15 interviews and began work to make them publicly available, including recruiting and placing photographs to enliven the written words.

Oral Histories in Directory of History of Medicine Collections
Oral histories are an important resource for historians and other scholars seeking to understand individual careers, the development of institutions and disciplines, and the process of biomedical research. You can find oral history collections around the world through the NLM Directory of History of Medicine Collections. Get Instructions for Searching.
Go To Directory
Rare books and journals.

A Shelflist of Islamic Medical Manuscripts (pdf)
In 1994, to celebrate the 900th anniversary of the oldest Arabic medical manuscript in its collection, the History of Medicine Division of the National Library of Medicine mounted an exhibition entitled Islamic Culture and the Medical Arts . Showcasing the library’s rich holdings in this area, the exhibit was very well received -so much so that there has been a scholarly demand for the library to issue a cataloge of its holdings. This shelflist serves as an interim guide to the collection.
VIEW EXHIBITION BROCHURE
View exhbition poster.

Islamic Medical Manuscripts
Here you can learn about Islamic medicine and science during the Middle Ages and the important role it played in the history of Europe. This site, with its biographies, colorful images, and extensive historical accounts of medieval medicine and science is designed for students and everyone interested in the history of Islamic and European culture. The site provides a comprehensive, annotated listing (including images) of the 300 or so Persian and Arabic manuscripts in the National Library of Medicine.

Early Western Manuscripts at NLM
The National Library of Medicine has in its collection 90 Western manuscripts written before 1601. Cataloging information for these manuscripts is fragmented and in some cases unavailable to the scholarly community. The following digitized pamphlet is available in the NLM’s Digital Collection.

Medieval Manuscripts
An interpretive overview of medieval manuscript holdings of the National Library of Medicine focused on medicine and medical literature in medieval England, on the sources and transmission of the manuscript texts, and on their later manifestations.

Time, Tide, and Tonics: The Patent Medicine In America
Almanacs, first produced in the middle ages for their astrological information, were, in the nineteenth century, adopted by patent medicine manufacturers to advertise their wares. By the end of the century they had evolved into colorful and heavily illustrated works, displaying catchy and clever cover art.
GENERAL REFERENCES
Index-catalogue of the library of the surgeon-general’s office.
The Index-Catalogue of the Library of the Surgeon-General’s Office ( Index-Catalogue ) is a multi-part printed bibliography or list of items in the Library of the Surgeon-General’s Office, U.S. Army, the National Library of Medicine’s earliest incarnation founded in 1865. It contains material dated from the 1400s through 1950 and is an important resource for researchers in the history of medicine, history of science, and for clinical research. NLM has scanned all 61 volumes of the printed Index-Catalogue and made them available in NLM Digital Collections grouped by series: Series 1 , Series 2 , Series 3 , Series 4 , and Series 5 . The originals may be consulted in the NLM Reading Room and at many large research and medical school libraries. This resource is also available as an online, searchable database: see IndexCat ™. Read more about Index-Catalogue on our blog Circulating Now .
Bibliography of the History of Medicine
Journal articles, book chapters, and conference papers and proceedings that were published from 1965–1993 are indexed in the Bibliography of the History of Medicine . The Bibliography , a printed version of the discontinued HISTLINE database, was published in six cumulative volumes (1965–1993), and is useful for pre-1993 material. The Bibliography can be consulted in the Reading Room and at many large research and medical school libraries.
Index Medicus
Index to journal articles in biomedical journals worldwide published from 1879–1927. For detailed information about Index Medicus please see Index Medicus Chronology (archived) .
PRINTED GUIDES TO NLM HOLDINGS
- Dorothy M. Schullian, A Catalogue of Incunabula and Manuscripts in the Army Medical Library , 1950
- Richard J. Durling, A Catalogue of Sixteenth Century Printed Books in the National Library of Medicine , 1967
- Peter A. Krivatsy, A Catalogue of Incunabula and Sixteenth Century Printed Books in the National Library of Medicine, First Supplement , 1971
- Peter A. Krivatsy, A Catalogue of Sixteenth Century Printed Books in the National Library of Medicine. First Supplement , 1971
- Peter A. Krivatsy, A Catalogue of Seventeenth Century Printed Books in the National Library of Medicine , 1989
- John B. Blake, Eighteenth Century Printed Books in the National Library of Medicine (1979)
- Stephen J. Greenberg, A Shelflist of Islamic Medical Manuscripts at the National Library of Medicine , 1996 ( Download PDF )
- Sarah L. Richards, Motion Pictures and Videocassettes about the Public Health Service and its Agencies , 1998 ( Download PDF )
NEW ACCESSIONS IN THE HISTORY OF MEDICINE

Recent Acquisitions
The National Library of Medicine is constantly developing its historical collections through generous donations , transfers from government entities, and purchases, which adhere to the Library’s Collection Development Policy and support its mission.
VIEW RECENT ACQUISITION NEWS ON OUR BLOG
Unprocessed archives & papers collections.

These lists represent brief descriptions of unprocessed collections, or unprocessed additions to collections, and is primarily for informational purposes only. There may be donor imposed restrictions, HMD imposed restrictions, or no descriptions of collection contents. Please contact the HMD Reference Staff regarding access to these collections.
Note on Access: The majority of these collections are stored offsite and require 30 days prior notice for service. Please contact the Associate Curator of Archives and Modern Manuscripts for access information.
View 1997–2015
View pre-1997, archive finding aid.

NLM Institutional Archives Collection
A descriptive online guide to the archival collections of the National Library of Medicine.
WEB ARCHIVES

Web Archives of NLM Websites
The National Library of Medicine’s websites represent a significant aspect of its institutional records and are being archived through the Library’s Web Archiving efforts.
View NLM INSTITUTIONAL WEB ARCHIVES
Digitized nlm publications and productions.

Selected digitized publications and productions of the National Library of Medicine including bibliographies, catalogs, posters, brochures, programs and audiovisuals relating to its collections, activities, and resources.
Go to NLM DIGITAL COLLECTIONS

Archives and Personal Papers Collections
Digitized archival collections, often en masse, from the holdings of the Archives and Modern Manuscripts collctions.
GO TO NLM DIGITAL COLLECTIONS

Student Lecture Notes
Digitized lecture notes from our bound manuscripts holdings. Largely dating from the 18th-19th centuries, these handwritten lecture notes are the recordings of in-class lectures as transcribed by students from some of the world's major medical schools of the time such as the University of Edinburgh, the University of Pennsylvania, and many others. Often produced as a graduation requirement, these volumes document the thoughts and teachings of American and European medical educators such as Benjamin Rush, Alexander Munro, and Philip Physick.

Recipe Books
Digitized recipe and cookery books from our bound manuscripts holdings. Often kept and maintained by female heads of households, these largely 18th century European handwritten works document both well-known and family recipies for medicinal compounds, remedies, and treatments for all types of ailments and bodily well-being, but also record general household needs such as food preparation and storage, plantings, herbals, and production of ink and paper.

NLM Publications and Productions
Publications and videos produced by NLM from NLM's institutional archives

Profiles in Science
Profiles in Science presents the lives and work of innovators in science, medicine, and public health through in-depth research, curation, and digitization of archival collection materials. NLM historians and archivists review and select documents from the Library's collections, and collaborating institutions, to bring the public biographical stories and direct access to supporting primary sources. Profiles in Science includes digitized letters, draft manuscripts, photographs, diaries, and more that provide insight into the challenges and successes of scientific discovery and the diversity of paths and perspectives involved.
View Collection

In His Own Words: Martin Cummings and the NLM
A searchable, online edition of annual Congressional appropriations testimonies and selected speeches and articles by former NLM director Dr. Martin M. Cummings, based on the collection of his papers (MS C 554; 116.0 linear feet) in the Library’s Modern Manuscripts collection. This project represents theNLM’s ongoing commitment to collecting materials related to its own institutional history—as part of the NLM Archives —as well as to digitizing these collections and making them widely available for the benefit of researchers, educators, and students.

FDA Notices of Judgment Collection, 1908–1966
The FDA Notices of Judgment Collection is a digital archive of the published notices judgment for products seized under authority of the 1906 Pure Food and Drug Act. This digital library, created using the SPER system, allows for browsing the collection as well as searching the collection’s metadata and full-text.

Physicians' Lives in the Shenandoah Valley: Henkel Family Letters, 1786–1907
The Henkel Family Correspondence collection consists of 828 letters and is largely the product of Caspar C. Henkel’s life. This digital edition is divided into 3 blog posts for ease of navigation and contextual narrative.
View Blog Posts on Circulating Now
Web collections.

Recognizing that web sites, blogs, social media, and other web content plays an increasingly important role in documenting the scholarly biomedical record and illustrating a diversity of philosophical and cultural perspectives in health and medicine, Archives and Modern Manuscripts has begun selectively collecting representative web content to augment our physical personal papers and organizational archives. NLM also periodically captures and archives large portions of its own web domain, including NLM blogs and social media. In addition to directly accessing archived web content through our Internet Archive Archive It service, archived websites are described in the pertinent collection finding aids.
MORE ABOUT WEB COLLECTING AND ARCHIVING AT NLM

Web collecting and archiving is the process of collecting web sites, social media, and other web content to ensure the information is preserved in an archive for future researchers, historians, and the public. NLM librarians and archivists use Archive-It web crawlers to collect web content guided by the Library’s collection development policies... Read More

Featured Collections
Explore a variety of curated history of medicine collections featuring supporting information and narratives.
GO TO Collections List

Historical Projects on MedlinePlus Topics
Explore intersections in historical and modern medicine through curated digital projects and MedlinePlus, a health information resource that provides extensive up-to-date information about diseases, conditions, and wellness issues.
GO TO Topics List

Browse NLM Exhibitions
Learn more about the National Library of Medicine’s exhibitions about the social and cultural history of medicine. Exhibitions include online education resources and in some cases Digital Galleries of materials from the NLM’s collection.
VIEW EXHIBITIONS
Traveling exhibitions.

Host NLM Traveling Exhibitions
Each year, hundreds of libraries and cultural institutions across the U.S. and around the world host NLM traveling exhibitions.
GO TO HOST NLM EXHIBITIONS
Exhibition program.

About the Exhibition Program
By creating exhibitions and educational resources about the social and cultural history of medicine, we encourage visitors of all ages to learn more about themselves and their communities. We seek to stimulate people’s enthusiasm for history and to nurture young professionals in history, education, museum studies, and the health professions.
GO TO EXHIBITION PROGRAM
Digitized materials pre-2000.

Brochures, catalogs, and other materials from exhibits at the National Library of Medicine held prior to 2000.
PUBLIC DOMAIN HISTORICAL IMAGES FROM NLM

Public domain images from the historical collections of the National Library of Medicine are accessible through The Commons on Flickr via a photostream . Among the hundreds of images available are book illustrations, photographs, fine art work, ephemera, and posters, including the 1918 World War I Red Cross nurse recruitment poster featured above. Visitors will also find albums (collections of images) including selections from the book Hidden Treasure , patent medicine trade cards, and AIDS posters. Visitors are encouraged to contribute information about images by adding comments and tags.
GO TO THE COMMONS ON FLICKR

Explore Options for Genealogical Research at NLM
The National Library of Medicine (NLM) is the largest medical library in the United States and is charged with preserving America’s medical heritage. The Library’s History of Medicine Division holds numerous genealogical and biographical resources, including manuscipt and archival collections, Medical School Bulletins and Catalogs, Printed Resources and the unique American Medical Association Deceased Physicians Master Card File .
GO TO GENEALOGY WEBSITE
Explore the papers of scientific leaders, view the collection, explore historical anatomical atlases.
Historical Anatomies
Historical Anatomies on the Web is a digital project designed to give Internet users access to high quality images from important anatomical atlases in the Library’s collection. The project offers selected images from NLM’s atlas collection, not the entire books, with an emphasis on images and not texts. However, links are provided to the full digitized book on NLM Digital Collections when available. Atlases and images are selected primarily for their historical and artistic significance, with priority placed upon the earliest and/or the best edition of a work in NLM’s possession.
LEARN MORE ABOUT USING HISTORICAL MATERIALS
Nlm historical collections copyright information.
Information about the copyright law of the United States as it applies to making reproductions of material found in the historical collections of the National Library of Medicine, with particular information about different formats including exhibitions, audiovisuals, images and other materials. If using any material from Historical collections for publication or production, please include the phrase: “Courtesy of the National Library of Medicine.”
Patron Guide to Copyright and Historical Materials
Patrons must make their own rights assessment in light of the intended use. The nature of historical archival collections means that copyright or other information about restrictions may be difficult or impossible to determine. The Library provides some information as a service to aid patrons in determining the appropriate use of an item, but that determination ultimately rests with the patron.
Last Reviewed: March 18, 2024

Founded in 1929, we are the oldest academic department of the History of Medicine in the English-speaking world. We are dedicated to scholarship on the histories of medicine, disease, the health sciences, and their relationships to society.
Latest News
Upcoming events.
No Events were found.
Announcements

We are committed to exploring the history of medicine in its broadest sense, both geographically and chronologically; we offer a range of graduate and undergraduate courses on topics such as the History of Chinese Medicine; Colonial Knowledge; Health and Healing in Early Modern England; Darwin, Freud, and Pasteur; and Disease Control in Historical Perspective.

The Institute of the History of Medicine is located in the William H. Welch Medical Library, named after the first Chair of the Department of the History of Medicine. In establishing the first Department of the History of Medicine in the English-speaking world, Welch sought to provide a humanistic component to medical education and public health.

The Department of the History of Medicine trains PhDs in the history of medicine, and teaches in the schools of medicine and public health. We offer courses for undergraduates and graduate students on the main arts and sciences campus of Johns Hopkins University.

The departmental library of the Institute, the Historical Collection is also the resource center for the history of medicine for the Hopkins community, and hosts visiting scholars from the United States and abroad. A research collection covering all aspects of the history of medicine, public health and allied sciences, it contains over 70,000 volumes. A large, comprehensive library of secondary sources accompanies a smaller, but choice collection of rare books, manuscripts, prints, photographs, medals, stamps and objects.

Meet our faculty, the largest department of medical historians in the US, staff, current graduate students, alumni, and postdoctoral fellows and visiting scholars from around the world.

The Bulletin of the History of Medicine is the official publication of the Johns Hopkins Institute of the History of Medicine and the American Association for the History of Medicine (AAHM) and is published by The Johns Hopkins University Press. A leading journal in its field for more than three quarters of a century, the Bulletin spans the social, cultural, and scientific aspects of the history of medicine worldwide.

The Department of the History of Medicine at Johns Hopkins, the first department of its type in North America, is proud to introduce new online CME modules that provide a historical perspective on issues of relevance to clinical practice today.
Insert/edit link
Enter the destination URL
Or link to existing content

Bulletin of the History of Medicine
Jeremy A. Greene, M.D., Ph.D., Johns Hopkins University; Alisha Rankin, Ph.D., Tufts University; Gabriela Soto Laveaga, Ph.D., Harvard University
Journal Details
The Bulletin publishes scholarly articles spanning the social, cultural, and scientific aspects of the history of medicine worldwide. Articles are based on historical research in primary sources grounded in the robust secondary literature in the history of medicine. Article submissions should clearly make critical interpretations and place the story in historical context. The Bulletin subscribes to the principles of the Committee on Publication Ethics ( COPE ). The Bulletin does not publish material that is available elsewhere, in any language, at the time of its publication in the journal, or material for which we must acknowledge permission to another publisher. We regularly publish articles that later appear as chapters in books, but the journal and its publisher, The Johns Hopkins University Press, hold the copyright, and the book publisher must request permission to reprint. Publication of the journal article must antedate publication of the book.
All new manuscripts must be submitted electronically at http://mc.manuscriptcentral.com/bhm . Authors should have no more than two manuscripts under review at any given time.
Conflicts of Interest : Authors are responsible for informing the editors of any institutional or organizational funding they have received for research related to the subject of the article.
The Wellcome Trust has changed its access policy concerning research articles that have been funded by the Trust. The new policy which became effective on January 1, 2021 can be found at: wellcome.org/grant-funding/guidance/open-access-guidance/open-access-policy .
Authors employed by NIH : The publisher and editors of the Bulletin understand that authors employed by NIH are obligated to post their articles in PMC. The Bulletin uses a two-step process in order to ensure that our authors can comply with this mandate. As is the case for most federal employee authors, the Bulletin cannot hold copyright of the article.
- Upon acceptance of an article by the Bulletin, the author should post a copy of the final manuscript of the essay to PMC specifying a 12-month embargo. The essay must be accompanied by the NIH publishing agreement and manuscript cover sheet and the Johns Hopkins University Press publishing agreement for U.S. Government employees, available from the editorial office. Copies of these documents should also be forwarded to the editorial office. Please note : the manuscript version of the essay is to be submitted to PMC in order for our authors to be in compliance, but the final PDF of the published essay is the version that will ultimately circulate on PMC.
- The BHM editorial office will take responsibility for posting the PDF of the final, published version of the article by the end of the 12-month embargo period, whereupon PMC will ignore the previously submitted unedited manuscript version of the essay. PMC will contact the author to confirm his or her permission to post the PDF version.
Preparing Your Manuscript for Submission
- BHM manuscripts should not exceed 12,000 words (including endnotes). Manuscripts over the word limit will not be considered.
- Double-space your manuscript: text, notes, and quotations.
- Use the same type size and font for all material.
- Quotations of more than six typed lines should be indented from the left margin and typed in a block format (double-spaced).
- Use American spelling.
- Dates should be written as, for example, “June 7, 2010.”
- To answer general questions about style and usage in BHM, refer to the Chicago Manual of Style (15th edition; CMS ).
- BHM requires numbered endnotes without a bibliography (See the CMS , 16th ed.).
- Document fully . BHM prefers to identify the source of each separate quotation with its own note; please do not bundle citations into a single note at the end of the paragraph. Please note that BHM requires inclusive page numbers for book chapters in edited collections and for all journal articles, in addition to page numbers for direct quotations. BHM uses abbreviations for journal names . For books and journals, follow the Bulletin examples given below; for more complex references, follow CMS .
Remember to provide: Full first names and middle initial(s) for authors and editors Subtitles of books and articles Full names of foreign journals cited Name of the publisher for books published after 1900 For newspaper articles, the author, title of article, and page numbers if available. Exact and inclusive page numbers for all quotations
The second and succeeding citations of references should refer back to the first full citation.
Citation Examples
1. Michael Worboys, Spreading Germs: Disease Theories and Medical Practice in Britain, 1865–1900 (Cambridge: Cambridge University Press, 2000), 81. [Book with page number for direct quotation]
2. Stephen Palmer, “Central American Encounters with Rockefeller Public Health, 1914–1921,” in Close Encounters of Empire: Writing the Cultural history of U.S.–Latin American Relations, ed. Catherine LeGrand, Gilbert Joseph, and Ricardo Salvatore (Durham, N.C.: Duke University Press, 1999), 311 – 32, quotation on 320. [Chapter in edited book with inclusive page numbers and page number for direct quotation]
3. Alexandra Stern, “Making Better Babies: Public Health and Race Betterment in Indiana, 1920–1935,” Amer. J. Public Health 90 (2002): 742 – 52, quotation on 751. [Journal article with inclusive page nos. and page no. of direct quotation.]
4. Ibid., 750.
5. Palmer, “Central American Encounters” (n. 2), 312. [Short form for previously cited item]
6. James Smith, “Public Health Experiments,” in LeGrand, Joseph, and Salvatore, Close Encounters (n. 2), 100 – 134. [Chapter in previously cited book]
7. Lauren Nauta, “Medical Development in New Jersey” (Ph.D. diss., University of Pennsylvania, 2006). [Dissertation]
Illustrations
- Illustrations are printed in black and white only. Photographs may be sent to the editorial office as glossy black-and-white 5” x 7” prints (do not send photos in color), or uploaded in TIFF or EPS formats. Halftones (art with any shades of grey) should be 266–300 dpi; line art, 900–1200 dpi. Do not use Word, PDF, or GIF files for illustrations.
- Indicate the approximate placement of all illustrations in the text. Provide captions for all tables and figures. Captions should include credit to the original sources.
Permissions
- You will need to provide copies of letters granting permission to reprint illustrations.
Unpublished theses present a particular problem. If you are quoting more than five sentences from such an unpublished work, please provide a letter granting permission from the author of the thesis or from the sponsoring university.
Uploading Your Manuscript
- At this time, ScholarOne cannot upload Word 2007 documents. Please save your manuscript as a Word 1997–2003 document before submitting.
- Please make sure to remove any identifying information (name, university, etc.) from the manuscript itself, as BHM reviews are double blind. Author acknowledgments are useful for the editorial office, but can also reveal the author’s institution or identity; therefore, please upload your acknowledgments in a separate file, selecting the file designation “Title Page” on ScholarOne Manuscripts.
- Please supply a required summary of 150 or fewer words with your paper.
- Please provide the required 4 to 8 keywords for indexing purposes.
The Hopkins Press Journals Ethics and Malpractice Statement can be found at the ethics-and-malpractice page.
Peer Review Policy
The Bulletin of the History of Medicine publishes scholarly articles spanning the social, cultural, and scientific aspects of the history of medicine worldwide. Articles are based on historical research in primary sources grounded in the robust secondary literature in the history of medicine. The Bulletin does not publish material that is available elsewhere, in any language, at the time of its publication in the journal, or material for which we must acknowledge permission to another publisher. We regularly publish articles that later appear as chapters in books, but the journal and its publisher, The Johns Hopkins University Press, hold the copyright, and the book publisher must request permission to reprint. Publication of the journal article must antedate publication of the book. In addition to offering new information based on scholarly historical research in primary sources, authors are expected to make critical interpretations and to place their narratives in a suitable historical and historiographic context. Authors must explain how their contribution fits in with the existing history of medicine literature on the topic at hand. Each article submitted for publication is assessed first by the editors (to make sure that it is a research article, and not a general overview of a subject), and then, if the article seems appropriate for the journal, by 3-4 historians expert in the particular area covered by the article. The journal utilizes a strict double-blind review process. If revisions are requested, the editors will decide which or all of the original reviewers to send the revised paper for re-reviewing. The approximate time between submission to initial decision is 4 months.
Dear xxxxxxx:
I am writing to request permission to reprint the illustration titled "xxxx." It appeared on page xx of (book or journal title), edited by xxxxx, in (year).This illustration is to appear as originally published [or with changes or deletions as noted] in "YOUR ARTICLE'S TITLE," by AUTHOR'S NAME, which the Johns Hopkins University Press is currently preparing for publication. This article is scheduled to be published in the MONTH, YEAR, issue of the Bulletin of the History of Medicine, in a press run of about 1,750 copies.I am requesting nonexclusive world rights to use this illustration in this journal in all languages and for all editions, in print and online, in all retrieval systems now or ever invented. Full acknowledgment will be given in the journal. Please sign below and return one copy of this letter to me to indicate your consent.If you don't hold the copyright to xxxx, or if I must seek permission from another source, please note the fact below. Should it be necessary for me to seek permission elsewhere, any information you could provide to help me contact the proper party would be greatly appreciated.Thank you for your consideration of this request.
The above request for permission to reprint is approved on the conditions specified below and on the understanding that full credit will be given to the source. The acknowledgment should read as follows:
Approved by:
Announcement from the Publisher
We have recently expanded the rights granted to contributors in our standard permissions agreement by allowing authors to include their articles in institutional depositories. Previously, the Press had restricted use to personal or departmental databases or on-line sites.
The change recognizes the important role institutions play in the scholarly communication process. It seems reasonable that the scholarship produced by faculty members should be made available to others within that same institution which, after all/ is providing either direct or indirect support.
The full text of the section that outlines author's rights is reproduced below. The new language is in point 4.
Rights of the Author: You have the following nonexclusive rights: (1) to use the Article in your own teaching activities; (2) to publish the Article, or permit its publication, as a part of any book you may write; (3) to include the Article in your own personal or departmental database or on-line site; (4) to include the article in your institutional database provided the database does not directly compete with either the Johns Hopkins University Press or Project Muse,is non-commercial, is institution-specific and not a repository that is discipline-based and/or accepts contributions from outside the institution. For use (4), you agree to request prior permission from the Press.
For all rights granted in this paragraph, you agree to credit the Press as publisher and copyright holder.
Special Issues
The Editors welcome proposals for special issues of the Bulletin that address themes of interest to the Bulletin 's wide-ranging readership—themes that go beyond a narrow time or place or topic and offer a rich array of perspectives and ideas. Successful special issues include a substantial introduction, written by the Guest Editor(s), that orients readers to the significance of the topic and situates the essays in the volume in a broad historiography of medicine, health, and healing.
A special issue can accommodate up to 10 articles, each with a maximum of 12,000 words of text (including footnotes). All special issue manuscripts are treated with the same protocol as regular Bulletin submissions: all manuscripts are sent out for peer review, where each essay is assessed by three external reviewers. (Please note: peer review will not commence until all special issue essays have been submitted.) The Editors make the final decision about publication but will consult with the Guest Editors as needed. A draft of the introduction may be reviewed by the Editors or sent to one or two scholars for comments and suggestions for improvement. Special issues are usually published approximately 12–18 months after manuscripts have been received. If, after peer review, only a few articles are accepted (~3), they can be published as a special section within a regular issue of the journal and include an abbreviated introduction. If fewer than three articles are accepted, they can be published in the Bulletin as regular articles.
Proposals should include : the names of the Guest Editor(s), a description and rationale for the issue (2-3 pp.), and a list of potential contributors and the titles and abstracts of their articles. The description and rationale should explain why the topic is (or should be) of interest to a broad array of historians of medicine. Proposals should be sent to the Editors at [email protected] .
Special Sections
A Bulletin special section can accommodate 3 articles, each with a maximum of 12,000 words of text (including footnotes), organized around a theme of interest to the journal’s readership. A short introduction should introduce the special section. All manuscripts are treated with the same protocol as regular Bulletin submissions: all manuscripts are sent out for peer review, where each essay is assessed by three external reviewers (peer review will not commence until all essays have been submitted). The Editors make the final decision about publication but will consult with the Guest Editors as needed. A draft of the introduction may be reviewed by the Editors or sent to one or two scholars for comments and suggestions for improvement. If fewer than three articles are accepted, they can be published in the Bulletin as regular articles.
Proposals should include : the names of the Guest Editor(s), a description and rationale for the section, and a list of potential contributors and the titles and abstracts of their articles. The description and rationale should explain why the topic is (or should be) of interest to a broad array of historians of medicine. Proposals should be sent to the Editors at [email protected] .
Forums can accommodate approximately 4-6 shorter essays (3,000-4,000 words, including footnotes). A Forum should be organized around a recognizable and coherent theme for which a Guest Editor should take responsibility (including an open call, if applicable). This flexible format allows for academic perspectives but also first-person perspectives. A short introduction should introduce the Forum. Forum pieces will not be subject to external peer review, but will be assessed by the Editors/Editorial Board. Editors make the final decision about publication but will consult with the Guest Editor(s) as needed. A draft of the introduction may be reviewed by the Editors or sent to one or two scholars for comments and suggestions for improvement.
Proposals should include : the names of the Guest Editor(s), a description and rationale for the Forum, and a list of potential contributors and essays. The description and rationale should explain why the topic is (or should be) of interest to a broad array of historians of medicine. Proposals should be sent to the editors at [email protected] .
Jeremy A. Greene Alisha Rankin Gabriela Soto Laveaga
Associate Editor
Carolyn McLaughlin
Advisory Editorial Board
Jacqueline Antonovich Catherine Burns Lara Freidenfelds Joseph Gabriel Lisa Haushofer Anne Kviem Lie Raúl Necochea López Abena Dove Osseo-Asare Deirdre Cooper Owens Akihito Suzuki Carsten Timmermann Dora Vargha
AAHM Officers
Barron Lerner, President Mary Fissell, Vice President Sarah Handley-Cousins, Secretary Scott Podolsky, Treasurer Keith Wailoo, Immediate Past President
AAHM Councilors
Adam Biggs Mary Augusta Brazelton Pablo F. Gómez Rana Hogarth Rebecca Kluchin Jessica Martucci Wangui Muigai Projit Bihari Mukharji Kelly O’Donnell Kavita Sivaramakrishnan Jacob Steere-Williams Harry Yi-Jui-Wu
The Bulletin of the History of Medicine regularly publishes reviews of a broad range of scholarly books in our field. The Editors carefully select potential reviewers whose scholarship allows for informed critiques of the books under review; this includes established historians and advanced PhD-level graduate students. The Editors also welcome proposals for book reviews, but the journal will not consider submissions of completed reviews prior to assignment. Reviewers will be asked to declare any potential conflicts of interest. Please contact the editorial office at [email protected] to discuss book review proposals.
Should you wish to be considered for a book review in the future, we would be happy to add you to our reviewer database. Please email a CV to the editorial office for consideration.
If you would like the Bulletin to review your book, please request that your publisher send a review copy to the editorial office below. Review copies received by the Johns Hopkins University Press office will be discarded.
The Editors Bulletin of the History of Medicine Johns Hopkins Institute of the History of Medicine 1900 East Monument Street, Rm. 306 Baltimore, MD 21205
Abstracting & Indexing Databases
- Bibliography of Asian Studies (Online), 1971-1992
- Arts & Humanities Citation Index
- Biological Abstracts (Online)
- BIOSIS Previews
- Current Contents
- Web of Science
- British and Irish Archaeological Bibliography (Online)
- Dietrich's Index Philosophicus
- IBZ - Internationale Bibliographie der Geistes- und Sozialwissenschaftlichen Zeitschriftenliteratur
- Internationale Bibliographie der Rezensionen Geistes- und Sozialwissenschaftlicher Literatur
- Academic Search Alumni Edition, 1/1/2003-
- Academic Search Complete, 1/1/2003-
- Academic Search Elite, 1/1/2003-
- Academic Search Premier, 1/1/2003-
- America: History and Life, 1/1/1963-
- Biography Index: Past and Present (H.W. Wilson), vol.76, no.1, 2002-vol.84, no.3, 2010
- Book Review Digest Plus (H.W. Wilson), Mar.2002-
- Current Abstracts, 1/1/2003-
- Gender Studies Database, 1/1/1940-
- General Science Abstracts (H.W. Wilson), 2002/03-
- General Science Full Text (H.W. Wilson), 4/15/2002-
- Historical Abstracts (Online), 1/1/1963-
- Library & Information Science Source, 4/1/1938-5/1/1939
- MLA International Bibliography (Modern Language Association)
- OmniFile Full Text Mega (H.W. Wilson), 4/15/2002-
- Public Affairs Index, 9/1/2003-
- Russian Academy of Sciences Bibliographies
- SocINDEX, 7/1/1973-
- SocINDEX with Full Text, 7/1/1973-
- STM Source, 9/1/2006-
- TOC Premier (Table of Contents), 1/1/2003-
- Women's Studies International, 1/1/1940-
- Scopus, 1945-ongoing
- Academic ASAP, 03/2002-06/2017
- Book Review Index Plus
- Gale Academic OneFile
- Gale Academic OneFile Select, 03/2002-
- Gale General OneFile, 03/2002-
- InfoTrac Custom, 3/2002-
- General Science Index, 2002/03-
- ArticleFirst, vol.64, no.1, 1990-vol.85, no.2, 2011
- Electronic Collections Online, vol.70, no.1, 1996-vol.85, no.2, 2011
- Personal Alert (E-mail)
- Health & Medical Collection, 4/1/2003-
- Health Research Premium Collection, 4/1/2003-
- Hospital Premium Collection, 4/1/2003-
- Medical Database, 4/1/2003-
- Periodicals Index Online
- Professional ProQuest Central, 04/01/2003-
- ProQuest 5000, 04/01/2003-
- ProQuest 5000 International, 04/01/2003-
- ProQuest Central, 04/01/2003-
- Research Library, 04/01/2003-
- Science Database, 04/01/2003-
- SciTech Premium Collection
- Abstracts in Anthropology (Online)
Abstracting & Indexing Sources
- Abstracts of Mycology (Ceased) (Print)
- Chemical Abstracts (Print) (Ceased) (Print)
- Index Medicus (Ceased) (Print)
- Index to Scientific Reviews (Ceased) (Print)
- Inpharma Weekly (Ceased) (Print)
- International Nursing Index (Ceased) (Print)
- Numismatic Literature (Ceased) (Print)
Source: Ulrichsweb Global Serials Directory.
1.0 (2022) 1.2 (Five-Year Impact Factor) 0.00102 (Eigenfactor™ Score) Rank in Category (by Journal Impact Factor): 22 of 48 journals, in “History & Philosophy of Science”
© Clarivate Analytics 2023
Published quarterly
Readers include: Historians, physicians, nurses, archivists, curators, librarians, and others interested in the social, cultural, and scientific aspects of the history of medicine worldwide
Print circulation: 881
Print Advertising Rates
Full Page: (4.75 x 7.5") - $575.00
Half Page: (4.75 x 3.5") - $431.00
2 Page Spread - $863.00
Print Advertising Deadlines
March Issue - January 15
June Issue - April 15
September Issue - July 15
December Issue - October 15
Online Advertising Rates (per month)
Promotion (400x200 pixels) - $431.00
Online Advertising Deadline
Online advertising reservations are placed on a month-to-month basis.
All online ads are due on the 20th of the month prior to the reservation.
General Advertising Info
For more information on advertising or to place an ad, please visit the Advertising page.
American Association for the History of Medicine
The Institute of the History of Medicine at Johns Hopkins University
The Bulletin’s online syllabus archive in the history of medicine
A blog about teaching the history of medicine.
The Bulletin provides blog posts on teaching resources in the history of medicine and maintains a syllabus archive at the blog, Recommended Dose at teachhistmed.com
eTOC (Electronic Table of Contents) alerts can be delivered to your inbox when this or any Hopkins Press journal is published via your ProjectMUSE MyMUSE account. Visit the eTOC instructions page for detailed instructions on setting up your MyMUSE account and alerts.
Also of Interest

Martha Montello, Harvard Medical School

Christopher Sogge, Johns Hopkins University

Anne Reinhardt, Williams College

Deborah Boyle, College of Charleston

Sandie Holguín and Jennifer Davis, University of Oklahoma

Georgia L. Irby, College of William & Mary

Clare Anderson, University of Leicester

Robin Mitchell-Boyask, Temple University

Rachel S. Harris, Florida Atlantic University

Melissa A. Wong, University of Illinois Urbana-Champaign

Steven Miles, Hong Kong University of Science and Technology

Bruce Holsinger, University of Virginia

Dr. Nora Gilbert, University of North Texas

Ellysa Stern Cahoy, Penn State University

Michael Blackie, University of Illinois at Chicago

Werdie van Staden, University of Pretoria, South Africa

Nicholas Morrow Williams, Arizona State University

James M. DuBois, Washington University in St. Louis; Ana S. Iltis, Wake Forest University; and Heidi Walsh, Washington University in St. Louis

Virginia M. Brennan, PhD, MA, Meharry Medical College

Ruth Oldenziel, Eindhoven University of Technology

Jane Hanenberg, Boston Psychoanalytic Society and Institute

Ari Kelman, University of California, Davis

Judah M. Cohen, Indiana University; Jessica Cooperman, Muhlenberg College; and Marni Davis, Georgia State University

A. Hal Strelnick, MD; Albert Einstein College of Medicine and Karen Calhoun, MA University of Michigan Institute for Clinical & Health Research

Leona Toker, The Hebrew University of Jerusalem

Sabine Huebner, University of Basel, Switzerland
Hopkins Press Journals

- Foundations
- Write Paper
Search form
- Experiments
- Anthropology
- Self-Esteem
- Social Anxiety
Medical Research History
Here is a collection of medical research history.
This article is a part of the guide:
- Semmelweis' Germ Theory
- History of Antibiotics
- Discovery Of Bacteria
- Who Discovered DNA?
- Discovery of Pasteurization
Browse Full Outline
- 1 Medical Research History
- 2 Andreas Vesalius
- 3 Discovery of Pasteurization
- 4 Discovery Of Bacteria
- 5 Semmelweis' Germ Theory
- 6 Who Invented Vaccination?
- 7 History of Anesthesia
- 8 Discovery Of X-Ray Beams
- 9 History of Antibiotics
- 10 Who Discovered DNA?
- 11 Human Genome Project

Ancient Medicine
The history of medicine is a long and distinguished one, as healers sought to alleviate illnesses and fix injuries since the dawn of humanity. Ancient Medicine includes shamen and pagan priests used a blend of rituals and medical techniques, to cure ailments.
Islamic Medicine
The Islamic Golden Age, spanning the 8th to the 15th Centuries, saw many great advances in science, as Islamic scholars gathered knowledge from across the known world and added their own findings. One of these important fields was Islamic medicine , which saw medical practice begin to resemble our modern systems.
Andreas Vesalius and Modern Human Anatomy
Before Andreas Vesalius , the human anatomy was not learned by studying or dissecting bodies. Much of the knowledge was fictional, chiefly contributed by Galen over a millennium ago.
Louis Pasteur is regarded as one of the greatest saviors of humanity. He made numerous discoveries but he is best remembered for his advocation of the germs theory and the following discovery of pasteurization .
Discovery of Bacteria
Antony van Leeuwenhoek is regarded as the father of microbiology. Van Leeuwenhoek is known for the discovery of bacteria .
Semmelweis and Hand Washing
Ignaz Semmelweis introduced hand washing standards after discovering that the occurrence of puerperal fever could be prevented by practicing hand disinfection in obstetrical clinics. He believed that microbes causing infection were readily transferred from patients to patients, medical staff to patients and vice versa.
Edward Jenner and Development of Vaccination
Edward Jenner developed and generalized the vaccination technique against the dreadful smallpox disease. Although he did not originate the idea of cowpox attack to confer immunity against smallpox, yet it was his experiments and investigations which transformed a traditional belief into standard procedure to save innumerable millions of lives.
The History of Anesthesia
Research on modern techniques to reduce surgical pain began when an English scientist Joseph Priestley (1733-1804) discovered that inhalation of nitrous oxide might relieve pain. This introduced the development of modern anesthesia .
The Discovery of X-Ray Beams
While Wilhelm Conrad Roentgen was experimenting, he observed that certain rays were emitted during the passing of the current through discharge tube. This discovery lead to the development of the X-ray.
The Discovery of Antibiotics
As a result of some intelligent serendipity, Alexander Fleming stumbled on discovering penicillin .
Who Discovered Dna?
Wilkins, Crick and Watson got the Nobel Prize for their DNA discovery and development of the DNA theory.
Human Genome Project
The Human Genome Project (HGP) was a collaborative scientific research program on international scale conducted to discover all the chemical base pairs which make up human DNA for further biological studies. Its primary goal was to map and identify both physically and functionally, the approximately 20,000-25,000 genes of the human genome.

Some of the Nobel Prizes in 'Medicine or Physiology'
1981 nobel prize in 'medicine or physiology'.
Discoveries Concerning the Visual System Winners: David H. Hubel and Torsten N. Wiesel
Functional Specialization of Cerebral Hemispheres Winner: Roger Sperry
1982 Nobel Prize in 'Medicine or Physiology'
Discovery of Prostaglandins Winners: Sune K. Bergstrom, Bengt I. Samuelsson & John R. Vane
1983 Nobel Prize in 'Medicine or Physiology'
Discovery of Mobile Genetic Elements Winner: Barbara McClintock
1991 Nobel Prize in 'Medicine or Physiology'
Discovery of the function and mechanisms behind ion channels in cells Winners: Erwin Neher & Bert Sakmann
1992 Nobel Prize in 'Medicine or Physiology'
Discovery of reversible protein phosphorylation Winners: Edmond H. Fischer and Edwin G. Krebs
1993 Nobel Prize in 'Medicine or Physiology'
Discovery that genes in higher organisms do not present as single, continuous strand DNA but rather, the genes present as segments Winners: Richard J. Roberts & Phillip A. Sharp
1994 Nobel Prize in 'Medicine or Physiology'
The Role of G-Proteins in Signal Transduction Winners: Alfred G. Gilman & Martin Rodbell
1995 Nobel Prize in 'Medicine or Physiology'
Discovery of the Genetic Control of Embryonic Development Winners: Edward B. Lewis, Christiane Nuesslein-Volhard and Eric F. Wieschaus
1996 Nobel Prize in 'Medicine or Physiology'
Discoveries of the specificity of the cell mediated immune defence Winners: Peter C Doherty and Rolf M Zinkernagel
1997 Nobel Prize in 'Medicine or Physiology'
Discovery of Prions - a new biological principle of infection Winner: Stanley B. Prusiner
1998 Nobel Prize in 'Medicine or Physiology'
Discoveries of nitric oxide as a signaling molecule in the cardiovascular system Winners: Robert F. Furchgott, Louis J. Ignarro and Ferid Murad
1999 Nobel Prize in 'Medicine or Physiology'
Discovery that proteins have intrinsic signals that govern their transport and localization in the cell Winner: Günter Blobel
2000 Nobel Prize in 'Medicine or Physiology'
Discoveries of signal transduction in the nervous system Winners: Arvid Carlsson, Paul Greengard and Eric R. Kandel
2001 Nobel Prize in 'Medicine or Physiology'
Discoveries of key regulators of the cell cycle Winners: Leland H. Hartwell, Tim Hunt and Sir Paul M. Nurse
2002 Nobel Prize in 'Medicine or Physiology'
Discoveries concerning 'genetic regulation of organ development and programmed cell death' Winners: Sydney Brenner, H. Robert Horvitz and John E. Sulston
2003 Nobel Prize in 'Medicine or Physiology'
Discoveries concerning magnetic resonance imaging Winners: Paul Lauterbur and Sir Peter Mansfield
2004 Nobel Prize in 'Medicine or Physiology'
Discoveries of odorant receptors and the organization of the olfactory system Winners: Richard Axel and Linda B. Buck
2005 Nobel Prize in 'Medicine or Physiology'
Discovery of the bacterium Helicobacter pylori and its role in gastritis and peptic ulcer disease Winners: Barry J. Marshall and J. Robin Warren
2006 Nobel Prize in 'Medicine or Physiology'
Discovery of RNA interference - gene silencing by double-stranded RNA Winners: Andrew Z. Fire and Craig C. Mello
2007 Nobel Prize in 'Medicine or Physiology'
Discoveries of principles for introducing specific gene modifications in mice by the use of embryonic stem cells Winners: Mario R. Capecchi, Sir Martin J. Evans and Oliver Smithies
2008 Nobel Prize in 'Medicine or Physiology'
Discovery of human papilloma viruses causing cervical cancer Winner: Harald zur Hausen Discovery of human immunodeficiency virus (HIV): The Cause of AIDS Winners: Françoise Barré-Sinoussi and Luc Montagnier
2009 Nobel Prize in 'Medicine or Physiology'
Discovery of how chromosomes are protected by telomeres and enzyme telomerase . Winners: Elizabeth Blackburn, Carol Greider and Jack Szostak.
- Psychology 101
- Flags and Countries
- Capitals and Countries
Oskar Blakstad (May 13, 2010). Medical Research History. Retrieved Apr 11, 2024 from Explorable.com: https://explorable.com/medical-research-history
You Are Allowed To Copy The Text
The text in this article is licensed under the Creative Commons-License Attribution 4.0 International (CC BY 4.0) .
This means you're free to copy, share and adapt any parts (or all) of the text in the article, as long as you give appropriate credit and provide a link/reference to this page.
That is it. You don't need our permission to copy the article; just include a link/reference back to this page. You can use it freely (with some kind of link), and we're also okay with people reprinting in publications like books, blogs, newsletters, course-material, papers, wikipedia and presentations (with clear attribution).
Want to stay up to date? Follow us!
Save this course for later.
Don't have time for it all now? No problem, save it as a course and come back to it later.
Footer bottom
- Privacy Policy
- Subscribe to our RSS Feed
- Like us on Facebook
- Follow us on Twitter
A Brief History of Human Challenge Trials
For more than two centuries, scientists have been intentionally infecting patients with dangerous diseases in order to learn more
Theresa Machemer
Correspondent
:focal(685x708:686x709)/https://tf-cmsv2-smithsonianmag-media.s3.amazonaws.com/filer/97/0f/970f0f9d-8d9e-4291-9a85-b4b743aa0a43/gettyimages-1230010833_web.jpg "medical research history")
Physicians promise in the Hippocratic oath to keep their patients from harm, so intentionally exposing people to a deadly disease would seem to run counter to that contract. But with human challenge studies, they do exactly that. In challenge studies, medical professionals purposefully expose patients to illnesses so that they can study the patient’s symptoms and immune system response. Such studies can also help physicians discover what vaccines will work to prevent the affliction. Historically in such experiments, the health of individual patients, usually voluntary but at times, horrifically, not, has been sacrificed for medical knowledge and future treatments.
Researchers are planning new human challenge trials as the race to develop vaccines against Covid-19 is in a full sprint, with Pfizer’s vaccine receiving authorization in several countries and Moderna’s not far behind. But the end of the pandemic won’t just come from these two pharmaceutical breakthroughs. In order to fully contain the spread of Covid-19, many treatments and vaccines may be necessary in order to vaccinate billions of people. And some experts say that the fastest way to test those second-generation vaccines is through human challenge trials.
Imperial College London intends to begin a human challenge study related to Covid-19 as soon as January. During the study, scientists would purposely infect up to 100 young, healthy volunteers with the coronavirus that causes Covid-19 in the hopes of accelerating the search for new vaccines.
Supporters of the controversial Covid-19 human challenge trial argue that if it can be done safely then it provides a uniquely controlled environment to study factors that are difficult to unravel in longer, large-scale Phase III trials of thousands of people. Critics say that challenge studies are either unnecessary because of vaccine successes so far, or should be put on pause until a later date when they can be run safely. Critics also point out that safety is a concern even for young volunteers because scientists do not know how to treat Covid-19 or what its long-term effects are, and evidence presented by the World Health Organization in September showed that at least a fifth of people between 18 and 34 who catch Covid-19 experience prolonged symptoms.
The debate over such a contentious experiment is nothing new. Human challenge trials are as old as inoculation itself. In 1796, English surgeon Edward Jenner tested the world’s first vaccine by exposing his gardener’s 8-year-old son to cowpox and then smallpox. Human challenge trials have since been used to study dozens of diseases from cholera to cancer, but early studies often put participants directly in harm’s way, not always with their knowledge.
Today, challenge studies undergo careful review by boards of experts before they can begin. A key requirement of an ethical study is that volunteers provide informed consent , proving that they understand the risks of joining a study. The first informed consent process was introduced more than a century after Jenner’s human challenge study.
In 1898, as the U.S. warred with Spain in Cuba, yellow fever —which can cause liver damage, nausea, high fever and bleeding—killed 13 times more soldiers than war wounds. So in 1900, the U.S. Army established a commission led by pathologist Walter Reed to figure out how yellow fever spread and how to stop it. Because only humans seemed to fall ill with the disease, Reed and three colleagues on the commission designed a human challenge study to test a leading theory of yellow fever transmission: mosquito bites.
Reed recognized that if he was correct, then the study itself would be incredibly risky. The need to expose volunteers to deadly disease would have to be weighed with the responsibility to keep the volunteers safe.
“The general that created the commission told Walter Reed… that he had to be absolutely sure that no harm would be caused to the volunteers,” says Enrique Chaves-Carballo , a historian of medicine at the University of Kansas. “He was pretty specific about that.”
To balance his superior’s order with the study’s inherent risk, the commission came up with a novel solution: the first informed consent contract. The commission created a document for volunteers to sign, stating that they understood the study’s risks. However, the form suggested that abstaining from the study was risky, too. The contract stated :
“The undersigned understands perfectly well that in the case of the development of yellow fever in him, that he endangers his life to a certain extent but it being entirely impossible for him to avoid the infection during his stay in the island, he prefers to take the chance of contracting it intentionally in the belief that he will receive from the said Commission the greatest care and the most skillful medical service.”
During the experiment, the scientists first allowed mosquitoes to bite yellow fever patients so the insects would pick up the disease. Then, they brought the mosquitoes to healthy volunteers, and allowed the mosquitoes to bite them. When volunteers fell ill, Reed scoured blood samples for the microbe causing their illness.
Those with yellow fever were prescribed complete bed rest and fasting except for “a few sips of champagne” and some pain medication, says Chaves-Carballo. Volunteers received a hefty payment of $100 in gold per mosquito bite, and another $100 if they fell ill.
In the first round of experiments, 11 volunteers got mosquito bites. Two fell ill, and survived. The third man to fall ill, Jesse W. Lazear, was one of the scientists running the study. He was bitten by accident and died of yellow fever 12 days later.
Though Reed considered ending the study after the death of his colleague, the commission instead named a sanitary station Camp Lazear in his honor. And by 1901 , Reed and the commission had shown through their mosquito bite experiments that the insects transmit yellow fever. Inoculation of more volunteers with yellow fever patients’ filtered blood samples showed that a virus causes the disease—making yellow fever the first human virus scientists discovered.
With the disease-causing culprit identified, Reed returned to George Washington University (then Columbian University) to teach, and other scientists picked up the search for a yellow fever vaccine. U.S. army physician William Gorgas and Cuban-born physician Juan Guiteras established an inoculation station for a new round of human challenge studies in Havana. They hoped to learn how to induce light cases of yellow fever with mosquito bites in order to give people immunity. More than 20 volunteers signed up for the first experimental inoculations in 1901, including the only woman to participate in the study, a military nurse named Clara Maass.
Maass was bitten five times without developing yellow fever, and received $100 to send home to her mother and nine siblings in New Jersey—a huge sum compared to her monthly pay of $30 .
Her sixth mosquito bite proved fatal. She and two other volunteers were infected with a particularly violent strain of the virus—the doctors didn’t know how to induce just light cases—and all three died in August of 1901.
“Some of the headlines of the newspapers are like, ‘Nurse Dies for a Hundred Dollars,’” says Chaves-Carballo. “People responded to the fact that she was a young nurse who was trying her best to help her family.”
/https://tf-cmsv2-smithsonianmag-media.s3.amazonaws.com/filer/3e/cc/3ecc2bca-8915-4c6c-bce7-b396fa7855fd/gettyimages-517447560_web.jpg "medical research history")
Public outcry in the U.S. brought the Havana experiments to an end. Maass’ death brought the study’s exorbitant pay under fire, as such a large incentive may have interfered with the participants’ ability to accurately weigh the risk of joining the study. The fact that the study was run by the U.S. Army, and Reed’s participants were members of the military, also brought into question the participants’ ability to freely opt out of the study, says Monica McArthur , pediatrician and infectious disease specialist at the University of Maryland School of Medicine’s Center for Vaccine Development and Global Health.
“In a lot of the studies early on, the Walter Reed experiment and other studies, used what we would now consider vulnerable populations,” people who couldn’t freely agree to participate or make a fully informed decision, says McArthur. “Prisoners, for example, could be enrolled in studies.”
A classic example of a challenge study that relied on a vulnerable population is the Tuskegee Syphilis Study. Beginning in 1932 , the U.S. Public Health Service recruited about 600 poor African American men from around Tuskegee, Alabama, for a study of how syphilis worsens over time. About two-thirds of the men had syphilis, but the study doctors informed them they had “bad blood.”
After receiving this phony diagnosis, the men were persuaded to join the study in exchange for free meals, hospital access and treatment for “bad blood” and other unrelated conditions. The scientists also provided participants a burial stipend that would be paid to their survivors after their deaths.
Only about half of the men with syphilis received a treatment that was usually prescribed in the 1930s: doses of toxic arsenic and mercury. The doctors subjected the participants to blood draws and spinal taps, and after they died of syphilis, autopsies, all in pursuit of more information about the natural course of the disease. The study lasted for decades, and even after the medical community established that penicillin could cure the disease in the 1940s the men did not receive the medication.
In 1972, journalist Jean Heller of the Associated Press brought the Tuskegee Syphilis Study to light and shared how the doctors involved in the study had deceived the men participating. By then, only 74 of the men with syphilis still survived. Public outrage shut the study down three months after the report.
While the Tuskegee Syphilis Study relied on participants who were already ill, other studies exposed otherwise healthy people to deadly diseases. For example, from 1955 to 1970, a pediatrician exposed more than 50 children with mental disabilities to hepatitis in order to identify different strains of the disease and eventually develop vaccines. The trial took place at Willowbrook State School, a home for children and adults with developmental disabilities in Staten Island, New York.
The school was overcrowded and had a lengthy waitlist for new patients. But the study’s principal investigator, Saul Krugman, offered several parents the opportunity to cut the line if they agreed to enroll their children in the study. Krugman told them that their children were likely to catch the disease at the facility anyway, but by joining the study, they would have access to cleaner facilities and a chance at an eventual vaccine.
“I did feel coerced,” said Diana McCourt, who enrolled her daughter in the Willowbrook study, to Forbes ’ Leah Rosenbaum. “I felt like I was denied help unless I took this [opportunity].”
The Willowbrook studies, which ended in 1970, revealed the existence of the A and B strains of hepatitis and sped up the development of a hepatitis B vaccine. But the studies progressed even as some in the medical community criticized Krugman’s methods. In 1966, anesthesiologist Henry K. Beecher published a landmark essay detailing 22 examples of ongoing unethical research on human subjects, including the Willowbrook hepatitis studies, in order to raise awareness and end unethical practices that continued despite the creation of international human experimentation guidelines—the Nuremberg Code in 1947 and the Declaration of Helsinki in 1964.
In addition to the Willowbrook study, Beecher highlighted one study in which melanoma, a serious form of skin cancer, was transferred from a woman to her mother “in the hope of gaining a little better understanding of cancer immunity.” The woman died on the same day that her mother was to receive the melanoma injection, so the doctors knew the cancer was deadly. Her mother died 451 days after receiving the injection.
Beecher concluded that an ethical approach to experimentation requires, first and foremost, the informed consent of study volunteers. “The difficulty of obtaining this is discussed in detail,” he writes, “But it is absolutely essential to strive for it for moral, sociologic and legal reasons. The statement that consent has been obtained has little meaning unless the subject or his guardian is capable of understanding what is to be undertaken and unless all hazards are made clear.”
Human challenge studies became less common after the 1970s with the conclusion of unethical studies that shocked the public. Since then, the Declaration of Helsinki has been amended seven times to clarify ethical standards for human experiments, most recently in October of 2013. The current declaration states that “While the primary purpose of medical research is to generate new knowledge, this goal can never take precedence over the rights and interests of individual research subjects.”
When run well, challenge studies are still uniquely able to provide clear data about infectious diseases. “They are now coming back in favor with very rigorous ethical principles in place,” adds McArthur.
The University of Maryland used human challenge studies in 2012 and 2013 to develop a vaccine for cholera , which was approved by the FDA in 2016. Cholera was an ideal candidate for a safe human challenge study because it is well understood by scientists, is reliably treatable with fluids and antibiotics, and has no long-term effects after the infection is gone.
Informed consent procedures have come a long way since Reed’s contract. Volunteers can ask questions and seek outside guidance, and must pass an assessment designed by the researchers to prove that they understand the risks of a study. And the volunteers have the power to quit. “Every time there’s an encounter with the volunteer, it’s reaffirming that the volunteer is still willing and able to participate,” says McArthur.
According to a statement by Imperial College London, which still needs to have its experimental plan approved by government regulators before researchers can begin recruiting participants, volunteers’ safety is the number one priority. “It would be nice to see exactly how [Imperial College London] explains the risks and benefits to those participating in this study,” says Chaves-Carballo.
Covid-19 is different from other challenge study diseases: Scientists have been studying it for less than a year, physicians have no approved treatments to intervene if a volunteer’s illness becomes severe, and early evidence suggests Covid-19 can cause long-term effects even in young, previously healthy people. The Imperial College London study aims to first identify the minimum dose of coronavirus necessary to cause disease. The study would use that dose of virus to study how vaccines work in the body to prevent Covid-19, to look at potential treatments and study the immune response. The biomedical community remains split on whether such a study should be run, given all of the unknowns around Covid-19.
When scientists develop second- and third-generation vaccines, a challenge study allows researchers to work with just 100 people instead of tens of thousands. That means fewer people are asked to go without the vaccine for the sake of research. And by waiting to conduct a challenge study on Covid-19 until a later date, researchers might get access to new information about risk factors for severe disease, which could help make the study safer.
“I am not a fan of SARS-CoV-2 challenge studies,” says McArthur. “But if I’m playing devil’s advocate against myself, some of the very reasons [not to do a challenge study] that I listed might be reasons that someone else might say that a challenge study is beneficial. Because we don’t know that much about a disease, so we could learn more about it.”
Get the latest Science stories in your inbox.
Theresa Machemer | READ MORE
Theresa Machemer is a freelance writer based in Washington DC. Her work has also appeared in National Geographic and SciShow. Website: tkmach.com
- Research at Stowers
Technology Centers
- Publications
- Education & Outreach Education & Outreach
- Postdoc Community at Stowers
- Our Research Campus
- Our Satellite Lab at MBL
- Kansas City Community
History & Mission
- American Century Investments
- Stowers Resource Management
- Leadership & Member Support
- For Journalists
The Stowers Institute is a place where scientists can openly pursue and discover the secrets of life. Thanks to the vision of our founders and our unique funding model, we can transform science, allowing the opportunity to expand and accelerate our understanding of human health and disease.
Our Mission & Values
The Institute’s mission is to make a significant contribution to humanity through medical research by expanding our understanding of the secrets of life and by improving life's quality through innovative approaches to the causes, treatment, and prevention of diseases.
At the Stowers Institute we value teamwork, collaboration, and creativity. Our science reflects the contributions of a wide array of individuals, technologies, and approaches that together produce innovative and impactful research.
Our History
The Stowers Institute for Medical Research was born from the vision of our founders, James E. Stowers, Jr., and his wife Virginia, who aspired to provide an environment of extraordinary scientific research.
Jim trained as a physician before launching and steadfastly nurturing American Century Investments into a highly successful, global asset management firm. Virginia had a career as a registered nurse. So, the couple had a profound understanding of the role that foundational biomedical research plays in generating new therapies and saving lives.
But it was their personal experiences with cancer that solidified their decision in 1994 to dedicate their personal fortune toward creating one of the world’s most influential centers for foundational research.
Over the next decade, our founders endowed the Institute with gifts totaling over $2 billion, and established a funding model whereby the science is funded through the dividends from American Century Investments, placing these visionary philanthropists in the top ranks of the world’s most generous givers.
Today, more than two decades later, their vision has become a remarkable reality. And with the same pioneering spirit of our founders, Stowers scientists are catalysts for discoveries that are transforming our understanding of human health and disease.
Quick Facts
Principal Investigators
Ongoing research projects
Acre campus
Predoctoral Researchers
Postdoctoral Researchers
Research Training Programs
National Academy of Sciences Members
American Academy of Arts and Sciences Fellows
American Association for the Advancement of Science Fellows
Spent on research to date
Researchers and support staff
Get to know our Founders
Jim Stowers
Leaving an enduring legacy
From medical school to mutual funds to world-class science, Jim Stowers led a remarkable life.
Virginia Stowers
Dedicated to a life of service
Virginia’s determination for the Institute to succeed was drawn from her family’s battles with cancer. She envisioned the Institute as one of the most innovative and effective research organizations in the world.
Affiliated Organizations
Jim Stowers Jr. founded American Century Investments in 1958 to help people improve their financial position. The small firm he started has grown into a leading, global asset management firm, serving financial intermediaries, institutions, and individuals.
In an unparalleled act of generosity and with their personal fortune, Jim and his wife, Virginia, founded and endowed the Stowers Institute for Medical Research and BioMed Valley Discoveries.
Jim and Virginia envisioned that the Institute would give rise to new insights into the processes underlying health and disease. To translate foundational research findings into potential cures, they established BioMed Valley Discoveries, a clinical state biotechnology company focused on addressing unmet patient needs across a wide spectrum of diseases.
Together, these organizations aspire to fulfill our founders’ vision of connecting health and wealth for the good of all.
Diversity, Equity, and Inclusion
We aim to make a significant contribution to humanity through medical research by pursuing world-class science and innovation. We believe the best way to achieve this is by valuing and celebrating a diverse mix of minds and talents.
We intensely focus on creating an environment where everyone, from any background, can do their best work. We are committed to building a collaborative community that is diverse by nature, equitable by choice, and inclusive by action because “The best is yet to be.” - Jim Stowers.
Newsletter & Alerts
Read article
Local News | Framingham Heart Study recognizes 75 years,…
Share this:.
- Click to share on Facebook (Opens in new window)
- Click to share on Twitter (Opens in new window)
- Click to share on Reddit (Opens in new window)
- Click to print (Opens in new window)
- Your Tax Dollars
- Massachusetts
Local News | Framingham Heart Study recognizes 75 years, three generations of groundbreaking cardiovascular research
The study is now the longest running cohort study in the history of biomedical research.
")
The Framingham Heart Study has now spent 75 years radically transforming how the field of medicine understands heart disease, researchers and participants recognized Monday — with three generations of participants in the small city saving and improving countless lives across the globe.
“Much of what we’ve learned specifically from this study has become common knowledge,” said Monica Bertagnolli, director of the National Institutes of Health.
“Americans, not just their doctors now understand the risk factors for heart disease, among them high blood pressure, high cholesterol, smoking, physical inactivity, unhealthy diets, unhealthy weight,” the NIH director added. “And just as important, we’ve also learned that we can change these risk factors, and if we do it saves lives.”
Researchers, doctors and participants gathered in Framingham on Monday to celebrate the 75th anniversary of the monumental research study, now the longest running cohort study in the history of biomedical research.
The study began in 1948 with just over 5,200 men and women from Framingham participating and is now on its third generation of over 15,400 participants, many of them descendants from original participants.
It has reshaped how the medical field understands heart health and cardiovascular disease, notably giving rise to the understanding of risk factors and preventative treatment.
The Framingham Heart study has become a “must read” for students in the medical field, speakers said, and is only continuing to grow and give researchers robust data to understand brain, lung, liver, kidneys, lungs and more. Public officials applauded the participants for their enormous contribution to the field.
“It’s just huge to be a part of it, to be part of history, to be part of something so worldwide,” said Philip Ottaviani, a third generation participant and City Council chair. “It put us on the map.”
Ottaviani noted that his daughter will be a part of the fourth generation, carrying on a long legacy of the study.
The study has become an integral part of the Framingham community and the local history and culture, participants said.
“My parents thought it was so important and were so dedicated to it,” said Richard Tirrell, who was recruited into the second generation of the study as a 21-year-old and has participated for nearly 60 years. “And we knew neighbors, other people who were also members and the children of members who thought it was important.”
The original generation of the study really cut a cross section of the town — “doctors and lawyers and factory workers, milk men and housewives and nuns from schools” — and so many children in his generation were sold because of the experiences and the belief of their parents, Tirrell said. It all brought together a wide ranging group in a common mission.
“It was not just us, it was a group of interrelated people who all were dedicated to the proposition that we’re doing good,” Tirrell explained.
“It’s a good thing to do,” said Anne Nicholson, an original member of the Omni Cohort of the study, which expanded the research to better study participants of minority races in 1994. “I really do love it.”
The work of the study is far from over, speakers said. Though the risk of cardiovascular disease and death rates dropped by about 75% between the 1950s and 2010, the reduction hasn’t kept up since, said Dr. David Goff, NIH director at the Division of Cardiovascular Sciences and National Heart, Lung, and Blood Institute.
The trend is “quite troubling,” Goff said, with rates of heart disease going up, including for young and middle age adults. Some attribute the trend to the obesity and diabetes epidemics in the country.
“New times and new challenges call for new science,” said Goff. “The important work that’s going on here in Framingham, I would say has never been more important than it is today.”
More in Local News

Crime & Public Safety | Massachusetts woman crashes SUV into pot shop, injuries reported

BC blanks Michigan, advances to college hockey national title game

Boston University falls in Frozen Four semifinal on Denver’s OT goal

Crime & Public Safety | Karen Read motion to dismiss unsealed in massive document dump ahead of murder trial
This paper is in the following e-collection/theme issue:
Published on 8.4.2024 in Vol 10 (2024)
Importance of Patient History in Artificial Intelligence–Assisted Medical Diagnosis: Comparison Study
Authors of this article:
- Fumitoshi Fukuzawa 1 , MD ;
- Yasutaka Yanagita 1 , MD, PhD ;
- Daiki Yokokawa 1 , MD, PhD ;
- Shun Uchida 2 , MD ;
- Shiho Yamashita 1 , MD ;
- Yu Li 1 , MD, PhD ;
- Kiyoshi Shikino 1 , MD, MHPE, PhD ;
- Tomoko Tsukamoto 1 , MD, PhD ;
- Kazutaka Noda 1 , MD, PhD ;
- Takanori Uehara 1 , MD, PhD ;
- Masatomi Ikusaka 1 , MD, PhD
1 Department of General Medicine, Chiba University Hospital, , Chiba-shi, , Japan
2 Uchida Internal Medicine Clinic, , Saitama-shi, , Japan
Corresponding Author:
Fumitoshi Fukuzawa, MD
Background: Medical history contributes approximately 80% to a diagnosis, although physical examinations and laboratory investigations increase a physician’s confidence in the medical diagnosis. The concept of artificial intelligence (AI) was first proposed more than 70 years ago. Recently, its role in various fields of medicine has grown remarkably. However, no studies have evaluated the importance of patient history in AI-assisted medical diagnosis.
Objective: This study explored the contribution of patient history to AI-assisted medical diagnoses and assessed the accuracy of ChatGPT in reaching a clinical diagnosis based on the medical history provided.
Methods: Using clinical vignettes of 30 cases identified in The BMJ , we evaluated the accuracy of diagnoses generated by ChatGPT. We compared the diagnoses made by ChatGPT based solely on medical history with the correct diagnoses. We also compared the diagnoses made by ChatGPT after incorporating additional physical examination findings and laboratory data alongside history with the correct diagnoses.
Results: ChatGPT accurately diagnosed 76.6% (23/30) of the cases with only the medical history, consistent with previous research targeting physicians. We also found that this rate was 93.3% (28/30) when additional information was included.
Conclusions: Although adding additional information improves diagnostic accuracy, patient history remains a significant factor in AI-assisted medical diagnosis. Thus, when using AI in medical diagnosis, it is crucial to include pertinent and correct patient histories for an accurate diagnosis. Our findings emphasize the continued significance of patient history in clinical diagnoses in this age and highlight the need for its integration into AI-assisted medical diagnosis systems.
Introduction
Over the past decade, medical knowledge and diagnostic techniques have expanded globally and have become more accessible with remarkable advancements in clinical testing and useful reference systems. Despite these advancements, misdiagnosis significantly contributes to mortality, making it a significant public health issue [ 1 , 2 ]. Studies have shown discrepancies between clinical and postmortem autopsy diagnoses in at least 25% of patients [ 3 - 7 ]. One study suggests that approximately 40,500 adult patients in intensive care units in the United States die of misdiagnoses annually, and the predicted prevalence of potentially lethal misdiagnoses is 6.3% [ 8 ]. Another report suggests that diagnostic errors contribute to approximately 10% of deaths and 6% to 17% of hospital adverse events, and are the leading cause of medical malpractice claims [ 7 ]. Considering the operative characteristics of clinical investigations combined with the inherent variability in disease presentation, it is often challenging to diagnose patients correctly—an issue that has concerned physicians perennially. Decades ago, a pivotal study proposed that patient history contributes to approximately 80% of the diagnostic process [ 9 , 10 ]. Medical history remains crucial for diagnosis [ 11 , 12 ] and is vital in contemporary physicians’ clinical diagnoses.
With the advent of artificial intelligence (AI) in recent years, numerous studies have focused on AI-assisted diagnoses, including cancer screening and treatment [ 13 - 15 ], diagnostic ultrasound imaging [ 16 - 19 ], x-ray imaging [ 20 ], computed tomography [ 21 ], magnetic resonance imaging [ 22 ], and endoscopy [ 15 , 23 ]. Other reports on AI-assisted imaging diagnoses include AI’s applications in radiology, pathology, and dermatological imaging [ 13 , 24 ]. There have also been reports on the use of AI in diagnosing specific conditions [ 25 - 27 ]. However, while several studies have reported that AI is useful in screening, diagnosing, and even treating certain medical conditions, to the best of our knowledge, no study has examined the importance of patient history in AI-assisted medical diagnosis. In addition, the extent to which AI considers patient history in its diagnostic processes remains to be fully understood.
This study aimed to investigate the importance of patient history in an AI-assisted medical diagnostic process aided by ChatGPT (version 4.0; June 2, 2023), one of the most well-known large language models that was released on March 14, 2023, to better understand the future of diagnostic medicine where AI is predicted to play an increasingly prominent role. Our study explored the contribution of patient history to AI-assisted medical diagnoses and assessed the accuracy of ChatGPT in reaching a clinical diagnosis based on the medical history that was provided. By reevaluating the significance of patient history, our study contributes to the ongoing discourse on optimizing diagnostic processes, both conventional and AI-assisted.
Study Design, Settings, and Participants
In our study, we used some of the 45 standardized clinical vignettes in The BMJ ( Multimedia Appendix 1 ) to evaluate the diagnostic and triage accuracy of web-based symptom checkers [ 28 ]. These vignettes were published on June 5, 2015. They offer a balanced set of cases, with 15 cases requiring immediate attention, 15 cases requiring consultation but not immediately, and 15 cases not requiring immediate attention or consultation. They were identified from various clinical sources, including materials used to educate health professionals as well as a medical resource website, with content provided by a panel of physicians. Researchers have used these clinical vignettes to evaluate the usefulness of web-based symptom checkers and self-triage [ 28 - 31 ]. We chose these vignettes because of their varied severity levels, their origins from multiple resources rather than just 1 resource, and their credibility, having been used in prior studies. They also include some of the most commonly observed conditions in outpatient settings. Of the 45 cases, we selected those that included physical examination findings, test data, and medical history and provided a single distinct diagnosis. As illustrated in Figure 1 , we excluded patients with no distinct diagnoses within the vignettes to serve as a reference (3 cases) and those who did not undergo any physical examination or laboratory tests (12 cases). Finally, the remaining 30 cases were used in this study.

Data Collection and Measurements
We assigned the correct diagnosis for each of these 30 cases to “Answer.” We then used the AI model, ChatGPT, to generate 2 diagnoses: the first, labeled “History,” was obtained by inputting only the medical history into ChatGPT; the second set, labeled “All,” was produced by inputting the medical history and all the other additional information in the clinical vignettes. Each time ChatGPT was prompted to generate a diagnosis, a separate chat window was used ( Multimedia Appendix 2 ). Thus, we used 2 chat windows for each case—one for the “History” diagnosis and the other for the “All” diagnosis. Additionally, the patients’ information was not inputted incrementally.
The concordance rate was assessed among “Answer,” “History,” and “All.” To extract a diagnosis from ChatGPT, we ended each input session with the phrase “What is the most likely diagnosis?” For both the “History” and “All,” the session was deemed complete when the AI returned the single most likely diagnosis. If ChatGPT suggested multiple diagnoses or indicated that it did not provide the most likely diagnosis, we repeated the process under the same conditions for a maximum of 5 attempts. Cases for which a single diagnosis could not be obtained even after 5 attempts were excluded without making further attempts.
Ethical Considerations
Our research does not involve humans, medical records, patient information, observations of public behaviors, or secondary data analyses; hence, it is exempt from ethical approval, the requirement of informed consent, and institutional review board approval. Additionally, as no identifying information was included, the data did not need to be anonymized or deidentified, and the need for compensation did not arise because no human participants were included in the study.
Data Analysis
Three board-certified physicians working in a medical diagnostic department at our facility assessed the concordance among the 3 AI-proposed diagnoses (“Answer,” “History,” and “All”). Of the 3 physicians, 1 is general medicine board–certified, 1 is internal medicine board–certified, and 1 is internal medicine–, general internal medicine–, and family medicine board–certified; their postgraduate education spanned 7, 9, and 11 years, respectively. A diagnosis was considered to match if at least 2 of the 3 physicians agreed upon the correspondence. Distinguishing between acute pharyngitis and acute upper respiratory tract infection necessitated determining whether to consider diseases resulting from similar pathologies as correct diagnoses. In contrast, for diseases that are essentially the same but have different nomenclatures, such as oral ulcers and canker sores, we considered them correct diagnoses.
Among the 30 cases, 19 patients were male and 11 were female, with ages ranging from 18 months to 65 years. In total, 12 individuals were younger than 20 years.
The results are shown in Table 1 . Cases 1-15 of the original vignette represent those requiring emergent care, cases 16-30 represent those requiring nonemergent care, and cases 31-45 represent those that are appropriate for self-care. A comparison with the correct diagnosis listed in The BMJ vignettes (labeled as “Answer”) showed that “Answer” and “History” coincided 76.6% of the time, while “Answer” and “All” had a concordance rate of 93.3%. Five (16.7%) patients could not be diagnosed on the basis of medical history alone but were diagnosed when additional information was provided. In 1 (3.3%) case, the diagnosis was different and incorrect under both conditions (“History” and “All”). In 1 (3.3%) case, the incorrect diagnosis was the same under both conditions (“History” and “All”).
a We repeated outputs until a single plausible diagnosis was made, with a maximum of 5 attempts.
b Matching answers between Answer and History: 23/30 (76.6%); median trial count 1 (Q1 1, Q2 1, Q3 1).
c Matching answers between History and All: 28/30 (93.3%); median trial count 1 (Q1 1, Q2 1, Q3 1).
d The output matched with that of “Answer.”
e N/A: not applicable.
f We attempted to obtain a diagnosis 5 times but failed.
g We attempted to obtain a diagnosis twice but failed.
Figure 2 presents details regarding the number of attempts required. On average, 1.27 attempts were needed for inputs involving only medical history followed by the question “What is the most likely diagnosis?” When all possible information, including physical examination findings and laboratory data, were inputted, followed by the same question, an average of 1.00 attempt was required. Regarding the 2 cases shown in Figure 2 that required 5 attempts, ChatGPT was unable to narrow down the diagnosis to the single most likely option. Consequently, these cases were counted as mismatches with the correct diagnoses listed in The BMJ vignettes.

Principal Findings
Despite the advancements in medical knowledge and diagnostic techniques, misdiagnosis remains a significant issue. AI has shown promise in the diagnosis and treatment of medical conditions; however, there is limited understanding of how AI uses patient history for diagnostic purposes. Our study aimed to investigate the extent to which AI (ChatGPT) can use information from medical history to accurately diagnose common diseases, which are frequently encountered in general outpatient, emergency, and ward management settings. Although some studies have investigated the accuracy of AI-based medical diagnosis, our study is novel because it emphasizes the importance of patient history. We compared the diagnostic accuracy of diagnoses made on the basis of only patient history and those made using all the information; this makes our study unique. To the best of our knowledge, no previous research has been conducted on this topic.
Our study investigated the role of patient history in AI-assisted medical diagnoses using ChatGPT. We analyzed 30 standardized patient vignettes from The BMJ to assess the concordance rates between AI-proposed diagnoses based on medical history only and those based on both medical history and additional information. Our results showed high concordance rates of 76.6% between the “Answer” and “History” groups, suggesting the importance of patient history in AI-assisted diagnoses and highlighting the potential of AI in improving diagnostic accuracy. This result is similar to that of a previous study that involved actual physicians instead of ChatGPT [ 9 , 10 ].
Characteristics of cases that did not lead to appropriate diagnoses based on history alone include, for instance, the following: an appendicitis case (case 2 in Multimedia Appendix 1 ) for which there was no documentation of pain migration in the medical history, a meningitis case (case 10 in Multimedia Appendix 1 ) wherein only headache and fever were documented, an otitis media case (case 16 in Multimedia Appendix 1 ) wherein only upper respiratory symptoms were recorded with no mention of ear-related symptoms, errors in identifying the causative agent in a case of acute gastroenteritis (case 27 in Multimedia Appendix 1 ), and an acute pharyngitis case (case 34 in Multimedia Appendix 1 ) that lacked the necessary medical history to determine the Centor score. Such omissions in the medical history could be considered contributing factors to the misdiagnoses. When physical findings and test data were added, an accurate diagnosis was achieved in 28 out of 30 cases (93.3%), showing a 16.7% increase in the accuracy rate. These two cases were of acute pharyngitis diagnosed as acute upper respiratory tract infection and Salmonella enteritis diagnosed as acute gastroenteritis. While we considered these incorrect diagnoses for the purpose of this study, they could have been deemed correct under certain criteria. Of the 7 cases that did not match between “Answer” and “History,” 6 were of infectious diseases (21 of 30 cases were of infectious diseases). These included cases where appendicitis was mistaken for acute gastroenteritis, acute otitis media and acute pharyngitis were mistaken for upper respiratory infections, and a Salmonella infection was mistaken for a Campylobacter infection. Physical examinations or tests may help identify the site of infection or pathogen in cases of intra-abdominal or head and neck infections.
There are situations in which physical examination and clinical test information may not be available in clinical settings. For instance, digital patient encounters owing to the impact of the COVID-19 pandemic often preclude physical examinations and clinical tests. The widespread use of telemedicine approaches in COVID-19 management, from screening to follow-up, has demonstrated the community’s acceptance and interest in telehealth solutions [ 32 ]. Moreover, even in face-to-face consultations, there are scenarios, such as in clinics, where detailed clinical tests may not be feasible depending on the setting. Furthermore, we cannot perform all physical examinations and tests on all patients. Therefore, we should consider potential differential diagnoses and decide which pertinent physical examinations or tests are the most suitable and should be performed. Most importantly, it has been reported that one rarely makes a correct diagnosis when one cannot make a differential diagnosis based on history [ 11 ]. In addition, accurately predicting the diagnosis based on medical history is associated with a higher diagnostic accuracy of the physical examination, whereas incorrect prediction of the diagnosis based on medical history is associated with a lower diagnostic accuracy of the physical examination [ 33 ]. Based on these findings and suggestions, medical diagnosis using ChatGPT is considered heavily dependent on history.
Using AI for diagnosis can enhance diagnostic accuracy by more efficiently collecting medical histories. For instance, diagnosing acute appendicitis is sometimes challenging. AI may face the same challenge as that observed when, in our study, AI mistakenly identified acute appendicitis as acute gastroenteritis. This misdiagnosis may have occurred because the case lacked specific medical histories characteristic of appendicitis, such as pain migration. By configuring AI systems to verify pain migration in patients with abdominal pain, especially for such common conditions, diagnostic precision may improve.
There are 2 possible limitations in our study. First, it remains unclear whether similar results could be obtained with other vignettes or actual patients. Unlike using preprovided vignettes, among which we included 30 cases, diagnosis can be more challenging in clinical settings because it requires taking a medical history from patients. We included 30 cases from among the vignettes, which include some of the most commonly observed conditions in the outpatient setting. Although covering all the existing conditions is not feasible, we do not know if the case volume in our study is sufficiently high. This study included relatively simple cases in which patients had very few comorbidities, potentially making the diagnosis less challenging. Moreover, patients with psychiatric conditions tend to present with complex and lengthy case histories, and the wording used by mental health clinicians may differ, be inconsistent, be vague, or fail to pinpoint a diagnosis. Our vignettes did not include a diagnosis of any mental illness. Due to the abovementioned reasons, our results may not apply to all clinical settings. Furthermore, when we consider what the patient reports, results may differ if languages other than English are used since ChatGPT does not recognize some languages, and each language may have its unique nuance. This highlights the importance of linguistic diversity and cultural context in AI applications, particularly in medical diagnoses where patient communication and history are critical. Future iterations of AI systems should aim to incorporate a broader range of languages and understand cultural nuances to ensure more accurate and inclusive diagnostic support. This idea is important in the context of health inequality. Furthermore, disparities in technology access may pose some challenges. Future research should address these barriers to ensure equitable access to AI-assisted diagnostic tools.
Second, we encountered cases where the input of medical history followed by the question, “What is the most likely diagnosis?” failed to yield a single most likely diagnosis even after 5 attempts, which could have introduced bias into our results, although we only had 2 such cases.
In the future, studies should focus on training AI by implementing evidence-based medical information, enabling it to present the underlying reasons and guidelines for diagnoses. In the event of a misdiagnosis, analyzing the process that led to the false diagnosis could be challenging in an AI-assisted medical diagnosis. Given the current situation where reflection on misdiagnoses is not always feasible, AI should be used as an auxiliary tool in medical diagnosis. This approach underscores the importance of AI, deeming it a support system rather than a definitive diagnostic solution. This area needs further investigation. Future studies should also verify our results with certain common conditions or diseases, such as the top 10 diseases identified in the Global Burden of Diseases study [ 34 ], potentially leveraging the benefits and limitations of AI-assisted medical diagnosis.
Conclusions
Relevant patient history is essential for AI-assisted diagnosis. The input of relevant patient history or the development of AI systems capable of obtaining comprehensive medical histories is vital for AI-assisted medical diagnosis. Furthermore, even in the modern era of advanced medical knowledge and clinical testing, the significance of patient history in diagnosis remains crucial.
Data Availability
All of our clinical vignettes, results, and prompts used are provided in Multimedia Appendix 1 .
Authors' Contributions
FF conceptualized the study, designed the methodology, collected the data, and drafted the manuscript. YY, DY, and SU conceptualized the study, designed the methodology, and reviewed and edited the manuscript. SY, YL, KS, TT, KN, TU, and MI conceptualized the study and reviewed and edited the manuscript. No generative artificial intelligence was used in writing the manuscript.
Conflicts of Interest
None declared.
Clinical Vignettes used in our study.
Explanation of the prompts we used in our study.
- Omron R, Kotwal S, Garibaldi BT, Newman-Toker DE. The diagnostic performance feedback “calibration gap”: why clinical experience alone is not enough to prevent serious diagnostic errors. AEM Educ Train. Oct 2018;2(4):339-342. [ CrossRef ] [ Medline ]
- Committee on Diagnostic Error in Health Care, Board on Health Care Services, Institute of Medicine, The National Academies of Sciences, Engineering, and Medicine. In: Balogh EP, Miller BT, Ball JR, editors. Improving Diagnosis in Health Care. National Academies Press; 2015. ISBN: 9780309377720
- Friberg N, Ljungberg O, Berglund E, et al. Cause of death and significant disease found at autopsy. Virchows Arch. Dec 2019;475(6):781-788. [ CrossRef ] [ Medline ]
- Shojania KG, Burton EC, McDonald KM, Goldman L. Changes in rates of autopsy-detected diagnostic errors over time: a systematic review. JAMA. Jun 4, 2003;289(21):2849-2856. [ CrossRef ] [ Medline ]
- Schmitt BP, Kushner MS, Wiener SL. The diagnostic usefulness of the history of the patient with dyspnea. J Gen Intern Med. 1986;1(6):386-393. [ CrossRef ] [ Medline ]
- Kuijpers C, Fronczek J, van de Goot FRW, Niessen HWM, van Diest PJ, Jiwa M. The value of autopsies in the era of high-tech medicine: discrepant findings persist. J Clin Pathol. Jun 2014;67(6):512-519. [ CrossRef ] [ Medline ]
- Ball JR, Balogh E. Improving diagnosis in health care: highlights of a report from the National Academies of Sciences, Engineering, and Medicine. Ann Intern Med. Jan 5, 2016;164(1):59-61. [ CrossRef ] [ Medline ]
- Winters B, Custer J, Galvagno SM, et al. Diagnostic errors in the intensive care unit: a systematic review of autopsy studies. BMJ Qual Saf. Nov 2012;21(11):894-902. [ CrossRef ] [ Medline ]
- Hampton JR, Harrison MJ, Mitchell JR, Prichard JS, Seymour C. Relative contributions of history-taking, physical examination, and laboratory investigation to diagnosis and management of medical outpatients. Br Med J. May 31, 1975;2(5969):486-489. [ CrossRef ] [ Medline ]
- Peterson MC, Holbrook JM, Hales DV, Smith NL, Staker LV. Contributions of the history, physical examination, and laboratory investigation in making medical diagnoses. Obstet Gynecol Surv. Oct 1992;47(10):711-712. [ CrossRef ]
- Gruppen LD, Palchik NS, Wolf FM, Laing TJ, Oh MS, Davis WK. Medical student use of history and physical information in diagnostic reasoning. Arthritis Care Res. Jun 1993;6(2):64-70. [ CrossRef ] [ Medline ]
- Tsukamoto T, Ohira Y, Noda K, Takada T, Ikusaka M. The contribution of the medical history for the diagnosis of simulated cases by medical students. Int J Med Educ. Apr 2012;3:78-82. [ CrossRef ]
- Chen ZH, Lin L, Wu CF, Li CF, Xu RH, Sun Y. Artificial intelligence for assisting cancer diagnosis and treatment in the era of precision medicine. Cancer Commun (Lond). Nov 2021;41(11):1100-1115. [ CrossRef ] [ Medline ]
- Mitsala A, Tsalikidis C, Pitiakoudis M, Simopoulos C, Tsaroucha AK. Artificial intelligence in colorectal cancer screening, diagnosis and treatment. A new era. Curr Oncol. Apr 23, 2021;28(3):1581-1607. [ CrossRef ] [ Medline ]
- Ochiai K, Ozawa T, Shibata J, Ishihara S, Tada T. Current status of artificial intelligence-based computer-assisted diagnosis systems for gastric cancer in endoscopy. Diagnostics (Basel). Dec 13, 2022;12(12):3153. [ CrossRef ] [ Medline ]
- Calisto FM, Santiago C, Nunes N, Nascimento JC. Breastscreening-AI: evaluating medical intelligent agents for human-AI interactions. Artif Intell Med. May 2022;127:102285. [ CrossRef ] [ Medline ]
- Zhou LQ, Wang JY, Yu SY, et al. Artificial intelligence in medical imaging of the liver. World J Gastroenterol. Feb 14, 2019;25(6):672-682. [ CrossRef ] [ Medline ]
- Peng S, Liu Y, Lv W, et al. Deep learning-based artificial intelligence model to assist thyroid nodule diagnosis and management: a multicentre diagnostic study. Lancet Digit Health. Apr 2021;3(4):e250-e259. [ CrossRef ] [ Medline ]
- Drukker L, Noble JA, Papageorghiou AT. Introduction to artificial intelligence in ultrasound imaging in obstetrics and gynecology. Ultrasound Obstet Gynecol. Oct 2020;56(4):498-505. [ CrossRef ] [ Medline ]
- Guermazi A, Tannoury C, Kompel AJ, et al. Improving radiographic fracture recognition performance and efficiency using artificial intelligence. Radiology. Mar 2022;302(3):627-636. [ CrossRef ] [ Medline ]
- Zhang K, Liu X, Shen J, et al. Clinically applicable AI system for accurate diagnosis, quantitative measurements, and prognosis of COVID-19 pneumonia using computed tomography. Cell. Jun 11, 2020;181(6):1423-1433. [ CrossRef ] [ Medline ]
- Gore JC. Artificial intelligence in medical imaging. Magn Reson Imaging. May 2020;68:A1-A4. [ CrossRef ] [ Medline ]
- Okagawa Y, Abe S, Yamada M, Oda I, Saito Y. Artificial intelligence in endoscopy. Dig Dis Sci. May 2022;67(5):1553-1572. [ CrossRef ] [ Medline ]
- Ramesh AN, Kambhampati C, Monson JRT, Drew PJ. Artificial intelligence in medicine. Ann R Coll Surg Engl. Sep 2004;86(5):334-338. [ CrossRef ] [ Medline ]
- Revilla-León M, Gómez-Polo M, Barmak AB, et al. Artificial intelligence models for diagnosing gingivitis and periodontal disease: a systematic review. J Prosthet Dent. Dec 2023;130(6):816-824. [ CrossRef ] [ Medline ]
- Chung H, Jo Y, Ryu D, Jeong C, Choe SK, Lee J. Artificial-intelligence-driven discovery of prognostic biomarker for sarcopenia. J Cachexia Sarcopenia Muscle. Dec 2021;12(6):2220-2230. [ CrossRef ] [ Medline ]
- Uzun Ozsahin D, Ozgocmen C, Balcioglu O, Ozsahin I, Uzun B. Diagnostic AI and cardiac diseases. Diagnostics (Basel). Nov 22, 2022;12(12):2901. [ CrossRef ] [ Medline ]
- Semigran HL, Linder JA, Gidengil C, Mehrotra A. Evaluation of symptom checkers for self diagnosis and triage: audit study. BMJ. Jul 8, 2015;351:h3480. [ CrossRef ] [ Medline ]
- North F, Jensen TB, Stroebel RJ, et al. Self-triage use, subsequent healthcare utilization, and diagnoses: a retrospective study of process and clinical outcomes following self-triage and self-scheduling for ear or hearing symptoms. Health Serv Res Manag Epidemiol. 2023;10:23333928231168121. [ CrossRef ] [ Medline ]
- Riboli-Sasco E, El-Osta A, Alaa A, et al. Triage and diagnostic accuracy of online symptom checkers: systematic review. J Med Internet Res. Jun 2, 2023;25:e43803. [ CrossRef ] [ Medline ]
- Radionova N, Ög E, Wetzel AJ, Rieger MA, Preiser C. Impacts of symptom checkers for laypersons’ self-diagnosis on physicians in primary care: scoping review. J Med Internet Res. May 29, 2023;25:e39219. [ CrossRef ] [ Medline ]
- Khoshrounejad F, Hamednia M, Mehrjerd A, et al. Telehealth-based services during the COVID-19 pandemic: a systematic review of features and challenges. Front Public Health. 2021;9:711762. [ CrossRef ] [ Medline ]
- Shikino K, Ikusaka M, Ohira Y, et al. Influence of predicting the diagnosis from history on the accuracy of physical examination. Adv Med Educ Pract. 2015;6:143-148. [ CrossRef ] [ Medline ]
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. Oct 17, 2020;396(10258):1204-1222. [ CrossRef ] [ Medline ]
Abbreviations
Edited by David Chartash, Gunther Eysenbach, Taiane de Azevedo Cardoso; submitted 12.09.23; peer-reviewed by Clarence Baxter, Hao Sun; final revised version received 31.01.24; accepted 15.02.24; published 08.04.24.
© Fumitoshi Fukuzawa, Yasutaka Yanagita, Daiki Yokokawa, Shun Uchida, Shiho Yamashita, Yu Li, Kiyoshi Shikino, Tomoko Tsukamoto, Kazutaka Noda, Takanori Uehara, Masatomi Ikusaka. Originally published in JMIR Medical Education (https://mededu.jmir.org), 8.4.2024.
This is an open-access article distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/4.0/ ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work, first published in JMIR Medical Education, is properly cited. The complete bibliographic information, a link to the original publication on https://mededu.jmir.org/ , as well as this copyright and license information must be included.

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Animals (Basel)
Animal Experiments in Biomedical Research: A Historical Perspective
Simple summary.
This article reviews the use of non-human animals in biomedical research from a historical viewpoint, providing an insight into the most relevant social and moral issues on this topic across time, as well as to how the current paradigm for ethically and publically acceptable use of animals in biomedicine has been achieved.
The use of non-human animals in biomedical research has given important contributions to the medical progress achieved in our day, but it has also been a cause of heated public, scientific and philosophical discussion for hundreds of years. This review, with a mainly European outlook, addresses the history of animal use in biomedical research, some of its main protagonists and antagonists, and its effect on society from Antiquity to the present day, while providing a historical context with which to understand how we have arrived at the current paradigm regarding the ethical treatment of animals in research.
1. Introduction
Animal experimentation has played a central role in biomedical research throughout history. For centuries, however, it has also been an issue of heated public and philosophical discussion. While there are numerous historical overviews of animal research in certain fields or time periods, and some on its ethical controversy, there is presently no comprehensive review article on animal research, the social controversy surrounding it, and the emergence of different moral perspectives on animals within a historical context. This perspective of animal use in the life sciences and its moral and social implications from a historical viewpoint is important to gauge the key issues at stake and to evaluate present principles and practices in animal research.
This review aims to provide a starting point for students and scholars—either in the life sciences or the humanities—with an interest in animal research, animal ethics, and the history of science and medicine. The reader interested in a more in-depth analysis on some of the topics reviewed is referred to the reference list for suggestions of further reading.
2. From Antiquity to the Renaissance
Humans have been using other vertebrate animal species (referred to henceforth as animals) as models of their anatomy and physiology since the dawn of medicine. Because of the taboos regarding the dissection of humans, physicians in ancient Greece dissected animals for anatomical studies [ 1 ]. Prominent physicians from this period who performed “vivisections” ( stricto sensu the exploratory surgery of live animals, and historically used lato sensu as a depreciative way of referring to animal experiments) include Alcmaeon of Croton (6th–5th century BCE) [ 2 , 3 ], Aristotle, Diocles, Praxagoras (4th century BCE), Erasistratus, and Herophilus (4th–3rd century BCE) [ 1 , 3 , 4 ]. The latter two were Hellenic Alexandrians who disregarded the established taboos and went on to perform dissection and vivisection on convicted criminals, benefiting from the favorable intellectual and scientific environment in Alexandria at the time [ 1 ]. All of these authors had a great influence on Galen of Pergamon (2nd–3rd century CE), the prolific Roman physician of Greek ethnicity who developed, to an unprecedented level, the techniques for dissection and vivisection of animals [ 3 , 5 ] and on which he based his many treatises of medicine. These remained canonical, authoritative, and undisputed until the Renaissance [ 1 , 6 ].
For most ancient Greeks, using live animals in experiments did not raise any relevant moral questions. The supposed likeliness of humans to their anthropomorphic deities granted them a higher ranking in the scala naturae (“the chain of being”), a strict hierarchy where all living and non-living natural things—from minerals to the gods—were ranked according to their proximity to the divine. This view of humans as superior would later influence and underline the Judeo-Christian perspective of human dominion over all nature, as represented by texts by Augustine of Hippo (IV century) and Thomas Aquinas (XIII Century), the most influential Christian theologians of the Middle Ages. For Augustine, animals were part of a natural world created to serve humans (as much as the “earth, water and sky”) and humankind did not have any obligations to them. For Thomas Aquinas, the mistreatment of another person’s animal would be sinful, not for the sake of the animal in itself, but because it is someone else’s property. Cruelty to animals was nevertheless condemned by Aquinas, as it could lead humans to develop feelings and actions of cruelty towards other humans. Also, for this theologian, one could love irrational creatures for the sake of charity, the love of God and the benefit of fellow humans (for selected texts, see reference [ 7 ]).
The belief amongst ancient Greek physicians that nature could be understood by means of exploration and experiment—and the medical knowledge thus obtained to be of clinical relevance in practice—would be replaced by other schools of medical thought. Most notably, the Empiric school (3rd century BCE–4th century) would reject the study of anatomy and physiology by dissection of cadavers or by vivisection, not only on the grounds of cruelty and the established taboos, but also for its uselessness. Empiricists believed pain and death would distort the normal appearance of internal organs and criticized the speculative nature of the conclusions drawn from experiments. Indeed, and despite taking an experimental approach to understand the human body and illness, the interpretations of physiological processes made by ancient Greeks who performed vivisections were often inaccurate. The theoretical frameworks by which physicians interpreted their experiments more often than not led them to misguided conclusions. Observations would be understood in light of such paradigms as the Hippocratic theory of the four humors or the Pythagorean theory of the four elements, along with others of natural or supernatural basis, and to which they added their own theoretical conceptions and observational errors [ 1 , 4 , 6 , 8 , 9 ]. The study of human or animal anatomy and physiology was hence deemed irrelevant for clinical practice. Beginning with the decline of the Roman Empire and continuing throughout the Middle Ages, physiological experiments—along with scientific activity in general—would fall almost entirely into disuse and medical knowledge would become dogmatic. In an increasingly Christianized Europe, there was little motivation to pursue scientific advancement of medical knowledge, as people became more concerned with eternal life than with worldly life, and returned to Pre-Hippocratic beliefs in supernatural causes for disease and in the healing power of faith and superstition. Therefore, and despite medieval physicians’ reverence for Galen and his predecessors, the experimental approach used by these classical authors had been sentenced to oblivion [ 3 , 8 , 9 , 10 , 11 ].
The use of animal experiments to satisfy scientific enquiry would only re-emerge in the Renaissance. Flemish anatomist Vesalius (1514–1564), through the course of his work as a physician and surgeon, realized that many anatomical structures thought to exist in humans—on account of them being present in other animals—were in fact absent [ 6 ]. This led him to break the established civil and religious rules and dissect illegally obtained human cadavers, and publish very accurate descriptions of the human anatomy, which challenged the authority of the classical authors. As Herophilus did centuries before (but not carried on by his successors) [ 1 ] Vesalius would also examine the similarities and differences between the internal structure of humans and other animals, thus setting the foundations of modern comparative anatomy.
Alongside the progress in anatomical knowledge made possible by experimenters defying the Catholic Church’s opposition to the dissection of human bodies, the Renaissance period also witnessed the resurgence of vivisection as a heuristic method for the understanding of animal physiology. Vesalius would again recognize the value of physiological experiments on animals as both a learning and teaching resource—he would vivisect animals for medical students as the finishing touch at the end of his courses—a view shared by his contemporary, and presumable student and rival, Realdo Colombo (1516–1559) [ 3 ]. Later, Francis Bacon (1561–1626), considered by many the founder of modern scientific methodology, would also approve of the scientific relevance of vivisection, stating that “the inhumanity of anatomia vivorum was by Celsus justly reproved; yet in regard of the great use of this observation, the inquiry needed (…) might have been well diverted upon the dissection of beasts alive, which notwithstanding the dissimilitude of their parts may sufficiently satisfy this inquiry” [ 12 ].
3. Seventeenth Century and the Dawn of the Enlightenment
Physiological experiments on animals carried on throughout the seventeenth century, in the period favorable to scientific progress now known as the Age of Enlightenment. René Descartes’s (1596–1650) description of animals as “machine-like” [ 13 ] was heavily criticized by many of his contemporaries, but nevertheless provided scientists a way to justify what would now be considered extremely gruesome experiments [ 3 , 14 , 15 , 16 ] in a time when anesthesia, for humans and animals alike, was not available. It has been argued, however, that Descartes’s views on animals were misinterpreted [ 17 , 18 ]—misconstructions that may not always have been free from malice, either by his contemporaries [ 19 ] or present-day critics [ 20 ]—as he did not explicitly state that animals were incapable of feeling pain and indeed recognized them to be able to do so insofar as it depends on a bodily organ, and even admitted animals to be capable of such sentiments as fear, anger, hope or joy [ 13 ]. Nonetheless, regardless of it being misinterpreted or not (for a discussion see [ 21 ]), Cartesian machinism would be recurrently evoked in defense of vivisection in the 17th and 18th centuries [ 14 , 15 , 16 ]. Malebranche, following his interpretation of Descartes, would explicitly justify vivisection on the grounds of it only being “apparently harmful” to animals [ 3 , 15 , 22 ]. Also, as someone deeply interested in physiology and medicine [ 23 , 24 ], and a “man of his time,” Descartes performed vivisections himself [ 15 , 16 , 21 ], an activity for which his—perhaps more apologetic than wholehearted—view of animals as soulless, senseless automata “absolved man from the suspicion of crime” [ 25 ].
As for other contemporary philosophers, Baruch Spinoza (1632–1677) did not deny animals’ ability to feel, but considered we should nevertheless “use them as we please, treating them in a way which best suits us; for their nature is not like ours” [ 26 ], whereas John Locke (1632–1704) fully recognized that animals could feel and stated that children should be brought up to abhor the killing or torturing of any living thing in order to prevent them from later becoming capable of cruel actions to fellow humans [ 27 ]. Immanuel Kant (1724–1804) would reject Cartesian mechanistic views, thus acknowledging sentience to other animals. However, Kant would not extend his concept of human intrinsic and inalienable dignity to other species. In his Of Duties to Animals and Spirits , and mirroring Thomas Aquinas’s views on the subject, he observed that “all animals exist only as means, and not for their own sakes, in that they have no self-consciousness, whereas man is the end (…) it follows that we have no immediate duties to animals; our duties towards them are indirect duties to humanity” [ 28 ]. Kant believed his anthropocentric philosophy provided the moral tradition and contemporary thought of his society; it was a philosophical underpinning, rather than an abstraction distant from the thoughts and feelings of the ordinary man [ 29 ]. Indeed, his argument that cruelty against animals would lead to cruelty to humans was—as it continues to be—popular amongst the public and scholars (e.g., [ 30 ]). In Duties to Animals, Kant would refer to William Hogarth’s (1697–1764) popular series “The Four Stages of Cruelty” ( Figure 1 ), a set of four engravings that depicted how cruel actions against animals could lead to moral degradation and crime. Regarding animal use in research, Kant would state that “Vivisectionists, who use living animals for their experiments, certainly act cruelly, although their aim is praiseworthy, and they can justify their cruelty, since animals must be regarded as man’s instruments; but any such cruelty for sport cannot be justified” [ 28 ]. While he believed actions that offended human intrinsic dignity were unacceptable—no matter how laudable their ultimate purpose should be—when it came to animals it would not be the actions themselves, but rather their justification that defined the acceptability of those actions. While the Enlightenment marked the beginning of the departure from Christian theocentrism, in the new anthropocentric view, animals continued to have no moral standing on their own. In perspective, it should be noted this was a time in which the slave market thrived and women were seen as inferior. However, the recognition of animals’ sentience in the new philosophical thought would later be instrumental for new ethical perspectives to arise on the moral status of animals.

“First Stage of Cruelty” by William Hogarth (1750), the first plate from “The Four Stages of Cruelty” series, which describes the escalating violent behavior that follows childhood cruelty to animals to an adulthood of criminal life. In this scene, two boys plunge an arrow into the rectum of a dog, while another boy, most likely the pet’s owner, pleads with them to stop. Meanwhile, some boys are burning the eye of a bird, while others tie bones to a dog’s tail. Also, some boys play “cock-throwing” (a popular sport in eighteenth-century England, consisting of throwing stones or bottles at a cockerel tied to a stake) while others hang fighting cats, and others even throw animals from windows. Source: © Victoria and Albert Museum, London.
Amidst the list of notable Western seventeenth-century physiologists using animals, the most noteworthy was undoubtedly William Harvey (1578–1657), physician to kings James I and Charles I, and one of the founders of modern science. In 1628, his groundbreaking Exercitatio Anatomica de Motu Cordis et Sanguinis in Animalibus (“An Anatomical Exercise on the Motion of the Heart and Blood in Living Beings”) was published, in which he provided the most accurate description of blood circulation and heart function of his time [ 31 , 32 , 33 , 34 ]. Using the results of meticulously planned experiments on live animals, as well as their interpretation through mathematics and physics, in this treatise, Harvey disproved many of Galen’s fifteen-hundred-year-old ideas [ 35 , 36 ]. In the tradition of his own academic lineage (he studied in Parma with the renowned anatomist Fabricius, a pupil of Colombo), Harvey was also a prolific and skilled comparative anatomist, whose studies on the anatomy of animals included species of several taxa, including mammals, fish, amphibians, reptiles and even insects [ 37 ].
Harvey’s De Motu Cordis was highly criticized, since his experimental observations did not fit the prevalent theories of Western natural philosophy of his time (for an insight on the social, scientific and academic context surrounding Harvey see [ 33 , 37 , 38 ]), still heavily grounded on Galenic principles. Harvey’s findings would challenge firmly established beliefs, such as blood being continuously produced in the liver and transported through the veins to be consumed by other organs, while arteries were thought to be filled with air; the heart was believed to have a heating—rather than pumping—function, and blood was thought to flow between the ventricles across a permeable septum; the vascular system as a whole was thought to be open; the arterial and venous bloods were believed not to mix; and the mere concept of blood circulation was virtually unknown (however, his teacher Fabricius might already have envisaged the concept of blood circulation [ 34 ]. Also, blood circulation was already known in Chinese medicine sixteen centuries before Harvey [ 39 ]). From an epistemological point of view, such opposition also reflected a dispute between the empiricist and the rationalist approach to the understanding of nature, for Harvey professed “to learn and teach anatomy not from books but from dissection, not from the tenets of Philosophers but from the fabric of Nature” (from De Motus Cordi , cited in [ 32 ]). Not surprisingly, Descartes—although a researcher himself—disagreed emphatically with most of Harvey’s findings, since he believed that theories forged through philosophical reflection on metaphysics were superior to those resulting from experimental observation, thus considering experiments or interpretations that did not confirm his own natural philosophy as flawed [ 40 , 41 ]. He nevertheless praised Harvey’s discovery of circulation and the method of experiment and observation that had led to it, a support that would actually help to turn the tide amidst scholars in favor of Harvey’s observation-over-doctrine ideas and methodological approach on experimental physiology, thereby setting the ground for further developments in physiological knowledge [ 38 ].
Further advancements in physiology would be prompted by questions left unsolved by Harvey, many of them addressed by an ensemble of his colleagues and followers at Oxford who applied Harvey’s principle that life should be interpreted in light of new findings in physics in their physiological experiments on animals [ 42 , 43 , 44 , 45 ]. The Oxford Group included polymaths like Robert Hooke (1635–1703), John Locke (1632–1704), John Mayou (1640–1679), Richard Lower (1631–1691), Thomas Willis (1621–1675), Robert Boyle (1627–1691) and Christopher Wren (1632–1723), amidst several others. Most physiologists did not expect direct therapeutic applications to result from their experiments [ 45 ]. There were, however, a few exceptions, such as Lower’s attempts at intra and inter-species blood transfusions having in mind their medical application, or Johann Wepfer’s (1620–1695) use of animals as a proxy to humans to infer the toxicity of several substances [ 3 ], a practice that is still carried out to this day. Seventeenth-century physiology would mark the dawn of modern scientific inquiry in the life sciences. Animal experiments were now proving to be more informative and relevant for obtaining scientifically sound knowledge on basic biological processes than ever before. These advancements would eventually diminish the importance of Galenic dogmatic medicine—although some of its principles would still endure for many years—and ultimately pave the way for today’s evidence-based medicine.
The seventeenth century would also witness the advent of skepticism towards experiments on animals on scientific grounds. Physicians like Jean Riolan, Jr. (1580–1657) and Edmund O’Meara (1614–1681) began to question the validity of physiological experiments carried out on animals in such an extremely altered state as one endured under vivisection, although their hidden agenda was to restore the credibility of Galenic medicine [ 3 , 46 , 47 ]. This dispute between critics and advocates of the informative value of animal models of human physiology still echoes today, e.g., [ 48 ].
The moral acceptability of inducing suffering in animals on the physiologist’s workbench would also become an issue raised in opposition of vivisection before the end of the seventeenth century [ 3 ]. However, the acceptance of the animal-machine paradigm by many physiologists reassured them that their scientific undertakings were not cruel. Furthermore, even the many who acknowledged that animals suffered a great deal with experiments, nevertheless defended themselves against the accusation of cruelty by alleging that the suffering inflicted was not unjustified, but rather for the sake of humankind, in the same line of reasoning by which today animal research is still justified. Nevertheless, these scientists were often overwhelmed by the extreme ill treatment they forced themselves to carry out on fully conscious animals [ 3 , 45 , 49 ]. One such investigator was Robert Boyle, whose infamous experiments on live animals on an air pump (conceived by him and developed by Robert Hooke) consisted in registering how animals responded to increasingly rarefied air. While only two animal experiments in Boyle’s “pneumatic chamber” are described in his New Experiments Physico-Mechanical Touching the Spring of the Air and its Effects (1660)—he would nevertheless go on to publish further animal studies on physiology [ 50 , 51 ]. Public demonstrations of this experiment would become very popular in the eighteenth century, although it bore more of an entertaining, rather than educational, nature ( Figure 2 ).

“An Experiment on a Bird in an air pump”, by Joseph Wright of Derby (detail) (1768). In this brilliant artwork, the artist captures the multiple reactions elicited by the use of live animals as experimental subjects in eighteenth-century Britain, for which we can find a parallel in present day’s diverse attitudes on this topic, including shock, sadness, appreciation, curiosity and indifference. Currently in The National Gallery , London. Source: Wikimedia Commons .
4. Eighteenth Century and the Rise of Moral Consideration for Animals
Amongst the many remarkable physiologists of the eighteenth century, polymaths Stephen Hales (1677–1761) and Albrecht von Haller (1708–1777) stood out. Hales was responsible for the first measurement of pressure in the blood vessels, and for other important insights into cardiovascular and respiratory physiology [ 52 , 53 , 54 ]. He also gave landmark contributions to public health and other medical breakthroughs, including the invention of forceps. Von Haller was arguably the most prolific physiologist of his time, better known for his groundbreaking work on inflammation, neurophysiology, heart function, and hemodynamics [ 55 , 56 , 57 , 58 , 59 , 60 ]. Both researchers were disgusted by the gruesomeness of their own experiments and were concerned about their moral justification, but nevertheless carried on, certain of the need for the use of live animals for the comprehension of many basic physiological processes, which were yet far from being understood [ 3 , 49 , 61 , 62 ]. Other relevant landmarks of eighteenth-century biomedical science based on animal studies included the foundation of experimental pharmacology [ 63 ], electrophysiology [ 64 , 65 ], and modern embryology [ 66 ]. Despite these advancements in biological knowledge, the clinical relevance of animal studies continued to be challenged [ 3 , 61 , 62 ] and, indeed, direct benefits to human health from animal experiments would remain elusive throughout the eighteenth century [ 45 , 55 ] and well into the following century.
Opposition to vivisection had raised its tone since the beginning of the eighteenth century, prompted by the popularization of public displays of experiments on live animals—in particular the notorious demonstrations of Boyle’s notorious air pump experiments [ 3 , 61 , 62 ], which were seen as purposeless, and thus inherently cruel—but became more prominent in the second half of the century, particularly in northern Europe [ 3 , 61 , 62 , 67 ]. Anthropocentric views on human duties to animals began to become increasingly challenged by philosophers, from Voltaire’s (1694–1778) criticism of Cartesian machinism and the gruesomeness of animal experiments [ 68 ] to Jean-Jacques Rousseau’s (1712–1778), Jeremy Bentham’s (1748–1832) and Arthur Schopenhauer’s (1788–1860) criticism of those who viewed animals as mere “means to an end.” By referring to sentience rather than intelligence to grant animals inherent worth, these philosophers proposed a shift from an anthropocentric justification for our duties of kindness to animals, to human obligations towards other animals for the sake of the animals themselves [ 69 , 70 , 71 ]. Rousseau proposed that despite animals being unable to understand the concept of natural law or rights, they should nonetheless, as a “consequence of the sensibility with which they are endowed (…) partake of natural right.” While Bentham found the concept of natural right “nonsense” [ 72 ], he sanctioned the idea of granting animals moral standing for the sake of their sentience. As he would famously state: “The question is not, Can they reason? Nor, Can they talk? But, Can they suffer?” [ 71 ]. From his utilitarian philosophy standpoint ( i.e. , that a moral action is that which results in the highest overall wellbeing for all stakeholders), he deemed animal research acceptable, provided the experiment had “a determinate object, beneficial to mankind, accompanied with a fair prospect of the accomplishment of it,” thus admitting that humans had precedence over other animals, limited by the due consideration for their suffering [ 73 ]. Bentham’s utilitarianism continues to exert a great deal of influence in today’s debate on animal use in the life sciences.
Among philosophers and physiologists alike, the issue of discussion was now not if animals could feel or not and to what extent, but rather whether vivisection was justifiable based on the benefit for human beings derived from it. Thus, even when researchers had strong misgivings about the inflicted suffering of animals, benefit to humans remained a valid justification for them to pursue their scientific goals through vivisection [ 61 ]. While knowledge of bodily functions and pathology was still incipient at that time, eighteen-century physiologists differed from their seventeenth-century predecessors, as they believed that medical improvements could one day be achieved through advancing knowledge by the means of animal experimentation [ 62 ]. The same rationale—that human interests took precedence over animal suffering—would also be used by nineteenth-century physicians as an ethical justification for the use of animals.
5. The Nineteenth-Century Medical Revolution and the Upsurge of the Antivivisection Societies
By the beginning of the nineteenth century, medicine was undergoing a major revolution. The organization of medical practice was changing, with the construction of hospitals, the university training of medical doctors, and the invention of new instruments and methods for the medical profession [ 74 ]. There was also a growing acknowledgement by the medical community that most medical practice, up to that period, was based on unproven traditions and beliefs and that most therapies were not only ineffective but often worsened the patient’s condition. As a result, medical practice increasingly began to focus more on understanding pathology and disease progression, pursuing more accurate diagnosis and prognosis, and thus providing reliable and useful information to patients and families, as they realized this was often the best they could do at the time. This paradigm shift would help give more credit and recognition to medical doctors and scientists, who, at that time, were often viewed with disdain and suspicion by the general public. This gain in medical knowledge would, however, sometimes be at the expense of unapproved trials, invasive procedures, and no respect for what we would now call patients’ rights [ 75 , 76 , 77 ].
Another kind of medical revolution was taking place in the laboratories, one that would ultimately provide the consistent basic science on which twentieth-century modern medicine would set its foundations. This scientific revolution began with a political one. The French Revolution of the late eighteenth century would later, in the first-half of nineteenth century, set the grounds for the establishment of the Académie Royale de Médecine , a thriving academic environment where science—and physiology, chemistry, and pharmacy, in particular—would finally be incorporated into medicine. The acknowledgment of the great knowledge gap in physiology and pathology, and the openness to positivist views on scientific knowledge, led to the definitive abandonment of the quasi-esoteric and, up to that time, dominant vitalistic theories in physiology, which stated that a vital principle, the “soul”, was the main source of living functions in organisms, rather than biochemical reactions. This led to a generalization of the understanding of all bodily processes as an expression of physical and chemical factors, and to a greater relevance given to animal experiments for answering scientific questions ( Figure 3 ). At the Académie , animal experiments were being increasingly prompted by existing clinical problems, and carried out with the ultimate goal of developing new therapeutic approaches to tackle these issues. Importantly, the integration of veterinarians in the Académie was deemed valuable for their insight on such experiments [ 57 , 78 , 79 ]. Amidst many other prominent scientists, two physician–physiologists stood out for their contributions to experimental physiology, François Magendie (1783–1855) and, most notably, Magendie’s disciple, Claude Bernard (1813–1878) [ 67 , 80 , 81 , 82 , 83 , 84 ]. Bernard’s experimental epistemology, unlike his tutor’s more exploratory approach, advocated that only properly controlled and rigorously conducted animal experiments could provide reliable information on physiology and pathology of medical relevance, setting the landmark of experimental medicine [ 85 , 86 , 87 , 88 ]. Conciliating Descartes’s rationalism with Harvey’s empiricism, Bernard acknowledged the importance of ideas and theories for the formulation of hypotheses, safeguarding, however, that these were only useful if testable and only credible if substantiated through experimentation [ 80 , 89 ]. He seemed to have been aware of how important and groundbreaking his approach to medical knowledge would become, when in his opening remarks to medical students in his very first lecture he quoted himself from his seminal “Introduction to the Study of Experimental Medicine,” stating: The scientific medicine that I’m responsible to teach does not yet exist. We can only prepare the materials for future generations by founding and developing the experimental physiology which will form the basis of experimental medicine” [ 89 ].

“A physiological demonstration with vivisection of a dog,” by Émile-Édouard Mouchy. This 1832 oil painting—the only secular painting known of the artist—illustrates how French scholars valued physiological experimentation in service of scientific progress [ 90 ]. Notice how the struggling of the animal does not seem to affect the physiologist or his observers. Currently part of the Wellcome Gallery collection, London. Source: Wellcome Library .
From the 1830s and throughout the second half of the century, the concept of scientific medicine would also flourish amidst a distinct group of German/Prussian physiologists. Following the rationale that biology could be understood through the means of chemistry and physics, and through their pivotal animal experiments and the use of microscopy, these scientists vastly contributed to the development of anatomy, histology, pathology, embryology, neurophysiology, physiology and physics. The setting for this scientific and epistemological progress was the Anatomisches Museum in Berlin, where anatomist, zoologist, and physiologist Johannes Müller (1801–1858) offered workspace and supervision to brilliant students whose independent research he wished to encourage. Although lacking the money, space, and instruments available in the great German laboratories founded after 1850, the museum provided these young scientists—notably Theodor Schwann (1810–1882), Robert Remak (1815–1865), and Friedrich Henle (1809–1885) in the 1830s, and Carl Ludwig (1816–1895), Emil du Bois-Reymond (1818–1896), Ernst Brücke (1819–1892), Hermann von Helmholtz (1821–1894), and Rudolph Virchow (1821–1902) in the 1840s—a singular intellectual atmosphere for research. Henle and Virchow would become leaders of the 1840s’ medical revolution in Germany, promoting the reform of medicine by providing it with a scientific basis, while Brücke, Helmholtz, and Bois-Raymond’s focused on the development of physiology as an autonomous science [ 83 , 91 , 92 , 93 , 94 , 95 ]. Their contributions to medical knowledge through the nineteenth century, along with Magendie’s and Bernard’s pivotal works, would deeply influence their counterparts across the Western world in the latter decades of the nineteenth century. Thousands of students flocked to attend medical schools in Germanic universities (and French institutes, although to a lesser extent), many of them from across the Atlantic [ 85 , 88 , 91 , 96 , 97 ]. This, in turn, would lead to an unprecedented rise in animal research-based advancement in biological and medical knowledge in the late nineteenth century—with important consequences for public health and quality of life—as further discussed later in this text.
While the second half of the nineteenth century marked the beginning of scientifically meaningful and medically relevant animal research, this period also saw opposition to vivisection becoming a more widespread idea in Europe, especially in Britain. Although animal experiments were not yet regulated in the first half of the century, the development of British physiology research in the Victorian Era was losing pace to Germany and France, where unprecedented progress in medical knowledge was taking place. The openly antivivisectionist positions of influential jurists, politicians, literary figures, clergymen, distinguished members of the medical community, and even Queen Victoria, contributed to an unfriendly environment for animal-based medical research [ 90 , 91 ]. There was, however, also a matter of divergence of opinion between British anatomists and French physiologists on which was the best approach for obtaining medical knowledge. Taking advantage of the rising antivivisection trend, British anatomists explored the (undoubted) gruesomeness of Magendie’s experiments, along with some nationalistic partisanship and xenophobic feelings against France, in their defense of anatomical observation as the primary method for advancing physiology, to the detriment of experiment through vivisection. However, they seldom disclosed their own positive (or at least ambivalent) views on animal experiments as a means to corroborate findings achieved through anatomical exploration [ 90 , 98 , 99 ]. Magendie would become the arch-villain of the antivivisection movement. Despite the broad recognition of his contributions to science by most peers, he was also amongst the most infamous of his time for the disdain he held for his experimental subjects. This contestation was louder outside of France, where many of his fellow scientists, even those who approved of animal experimentation, described him as an exceptionally cruel person who submitted animals to needless torture [ 85 , 90 , 100 ]. His public presentations became the most notorious, particularly one he performed in England when he dissected a dog’s facial nerves while the animal was nailed down by each paw, and was left overnight for further dissection the following day [ 82 ]. A description of Magendie’s classes to medical students by an American physician added further to the widespread disgust directed towards his work:
This surgeon’s spring course of experimental physiology commenced in the beginning of April. I seldom fail of “assisting” at his murders. At his first lecture, a basketful of live rabbits, 8 glass receivers full of frogs, two pigeons, an owl, several tortoises and a pup were the victims ready to lay down their lives for the good of science! His discourse was to explain the function of the fifth pair of nerves. The facility was very striking with which the professor could cut the nerve at its origin, by introducing a sharp instrument through the cranium, immediately behind and below the eye. M. Magendie drew the attention of the class to several rabbits in which the fifth pair of nerves had been divided several days before. They were all blind of one eye, a deposition of lymph having taken place in the comes, from inflammation of the eye always following the operation alluded to, although the eye is by this section deprived of all its sensibility. Monsieur M. has not only lost all feeling for the victims he tortures, but he really likes his business. When the animal squeaks a little, the operator grins; when loud screams are uttered, he sometimes laughs outright. The professor has a most mild, gentle and amiable expression of countenance, and is in the habit of smoothing, fondling and patting his victim whilst occupied with preliminary remarks, and the rabbit either looks him in the face or ‘licks the hand just raised to shed his blood. During another lecture, in demonstrating the functions of the motive and sensitive fibers of the spinal nerves, he laid bare the spinal cord in a young pup, and cut one bundle after another of nerves. (…) Living dissection is as effectual a mode of teaching as it is revolting, and in many cases the experiments are unnecessarily cruel and too frequently reiterated; but so long as the thing is going on, I shall not fail to profit by it, although I never wish to see such experiments repeated. cit in Olmsted, 1944 [ 101 ]
All of Magendie’s experiments were carried out without anesthesia or analgesia (and animals would be left in agony for hours, or for students’ “hands-on” anatomical studies. While, in fairness, it should be recognized that anesthetics had not yet been discovered when Magendie performed the bulk of his work, even after this technique had become available, he and nearly all of his students continued to forgo anesthesia in their experiments [ 102 ]. Moreover, animal studies on the effects of anesthetics themselves (Bernard was responsible for significant contributions to the understanding of the physiology of anesthesia: for an overview, see references [ 103 , 104 ]) were performed, as well as anatomical studies that could well have been conducted with cadavers, with no need for animals to be exposed to such prolonged suffering. Magendie was so ill famed in Britain that his experiments were referenced in the House of Commons by Richard Martin (1754–1834) when he presented a bill for the abolition of bear-baiting and that would become the “Cruel Treatment of Cattle Act” of 1822, one of the first animal protection laws. He would be again evoked in the report favoring the regulation of animal experiments that led to the “Cruelty to Animals Act” of 1876, the first piece of legislation ever to regulate animal experiments. By that time, Magendie had been dead for over twenty years [ 82 , 90 , 100 ].
After Magendie’s death, the focus of antivivisectionists’ attention moved to Bernard’s works, which included cutting open conscious animals under the paralyzing effects of curare , or slowly “cooking” animals in ovens for his studies on thermoregulation [ 105 ]. Bernard’s line of work would eventually have a heavy personal cost. Tired of her husband’s atrocious experiments, his wife would divorce him—taking with her his two daughters, who grew up to hate him—and, joining the antivivisectionists’ ranks, set up rescue shelters for dogs. Even Bernard’s cause of death is attributed to years of work in a humid, cramped, and poorly ventilated laboratory. He would, however, die a national hero, being given the first state funeral ever to be granted to a scientist in France. In his later years, he would collect the highest academic and political honors, including a seat in the French senate [ 88 , 102 , 106 , 107 ].
Despite their utter disregard for animal suffering, Magendie and Bernard did not see themselves as the immoral senseless villains portrayed by their detractors, but rather as humanists. Indeed, their view that animals did not deserve the same moral consideration as humans made them condemn experiments in humans without previous work on animals, the general principle on which the use of animal models in biomedical science is still grounded. In a time when proper dosage, administration, and monitoring of anesthesia were still largely unknown, often leading to serious side effects and accidental deaths, Magendie would state, on the use of anesthetics in humans without previous and thorough tests on animals: “That is what I do not find moral, since we do not have the right to experiment on our fellows” [ 5 , 108 , 109 ]. The amorality of human experiments prior to animal testing in animals was also an ethical argument raised in favor of vivisection by Bernard [ 89 ], who wrote:
No hesitation is possible, the science of life can be established only by experiment, and we can save living beings from death only by sacrificing others. Experiments must be made either on man or on animals. Now I think physicians already make too many dangerous experiments on man, before carefully studying them on animals. I do not admit that it is moral to try more or less dangerous or active remedies on patients, without first experimenting with them on dogs; for I shall prove, further on, that results obtained on animals may all be conclusive for man when we know how to experiment properly. If it is immoral, then, to make an experiment on man when it is dangerous to him, even though the result may be useful to others, it is essentially moral to do experiments on an animal, even though painful and dangerous to him, if they may be useful to man.
British physiologists often refrained from experimenting on mammals, mostly on account of the public’s opposition to the gruesomeness of continental physiologists’ experiments. However, with the publication of Bernard’s book (1868) and John Burdon-Sanderson’s Handbook for the Physiological Laboratory (1873), the scientific relevance of animal experiments became increasingly acknowledged, providing a utilitarian justification for vivisection, despite the harm endured by animals, eventually resulting in the rise in animal studies in medical schools in Britain in the 1870s [ 5 , 88 , 99 ]. Furthermore, by this time, anesthetics were already available and used by British physiologists, leading RSPCA secretary John Colam to state that “laboratory practices in England were very different indeed from [those] of foreign physiologists.” While the usefulness of anesthetics to chemically restrain animals was certainly advantageous for researchers, pain relief was most likely the major reason behind their ready adoption by many physiologists in Britain, as the paralyzing properties of curare were already known and used for this purpose. In fact, even before the solidifying of the antivivisectionist struggle, British physiologists had set themselves guidelines for responsible research [ 110 , 111 ]. Nevertheless, many researchers still found the analgesic and anesthetic effect of these volatile agents to be a source of undesired variability, thus avoiding their use altogether [ 99 , 105 ].
The upsurge of animal research in Britain was accompanied by an intensification of the antivivisectionist struggle. In 1875, the first animal protection society with the specific aim of abolishing animal experiments was founded: the Victoria Street Society for the Protection of Animals Liable to Vivisection (later known as the National Anti-Vivisection Society), led by Irish feminist, suffragist, and animal advocate Frances Power Cobbe (1822–1904). Vivisection became a matter of public debate, only matched in Great Britain that century by the controversy around the 1859 publication of Charles Darwin’s (1809–1882) On the Origin of Species , in which he presented a strong scientific rationale for the acknowledgement of our close kinship with the rest of the animal world, giving both physiologists and antivivisectionists a strong argument for their cause, depending on the perspective.
As the original argument of antivivisectionists that animal research was inacceptable because it did not provide useful medical knowledge began to lose strength (however, it remained a recurrent accusation against animal research, see, for instance, [ 112 ]), the discussion shifted towards preventing unnecessary harm, rather than questioning the scientific value of animal experiments [ 99 ]. On the other hand, the use of anesthetics now allowed British scientists to argue that most physiological experiments involved little, if any, pain [ 105 , 110 , 113 ]. While this made some antivivisectionists ponder about their own standing on the use of animals in research—namely those who opposed vivisection on the grounds that the intense and prolonged suffering endured by animals on the physiologist table was intolerable—many others felt that the most relevant value at stake was the preservation of each animal life in itself, questioning if human benefit was sufficient reason for sacrificing animals [ 99 , 110 ]. Moreover, the claim that animals were rendered senseless to pain gave carte blanche to many physiologists to use as many animals as they pleased for research, teaching, and demonstrations, despite anesthesia often being improperly administered, thus failing to prevent suffering for more than the brief initial moments. A famous quote by George Hoggan (a former vivisectionist who was appalled to witness Bernard’s experiments and who would later co-found the Victoria Street Society ) illustrates the relevance of the new ethical issues that emerged: “I am inclined to look upon anaesthetics as the greatest curse to vivisectible animals” [ 5 , 99 ].
In the last decades of the nineteenth century, all of today’s most relevant arguments on the debate surrounding the use of animals for scientific purposes were already in place, as well as most of the rhetoric and means of action in defense of each position. These views included outright abolitionism and, on the opposite pole, scientists demanding to be allowed to work without restrictions; non-scientists accusing researchers to be self-biased and unable to think ethically about their work and, on the other side of the barricade, researchers disdaining the authority of non-scientists to criticize their work; the benefit for humankind argument vs . the questioning of the scientific and medical value of animal research on scientific grounds; public demand for stronger regulation vs . researchers’ appeals for more autonomy, freedom, and public trust; advocates of the justifiability of only applied research (but not basic research) vs. apologists of the value of all scientific knowledge, see [ 105 , 112 , 113 ].
Just like today, there were also those who valued both animal protection and scientific progress and, recognizing that each side had both relevant and fallacious arguments, found themselves in the middle-ground, where they sought ways for compromise and progress. Amongst these, the most notable was Charles Darwin, known for his affection to animals and abhorrence for any kind of cruelty, but also for his commitment to scientific reasoning and progress [ 111 , 114 , 115 ]. Additionally, Joseph Lister (1827–1912), one of the most influential physicians of his time, would decline a request by Queen Victoria in 1875 for him to speak out against vivisection. Lister was one of the few British surgeons that carried out vivisection, albeit only occasionally, and was acquainted with some of the most eminent continental physiologists. In his response letter to the Queen, he pointed out the importance of animal experiments for the advancement of medical knowledge, stressed that anesthetics should be used at all times, and also denounced the ill treatment of animals in sports, cruel training methods, and artificial fattening of animals for human consumption as being more cruel than their use in research [ 116 ].
With the controversy assuming growing complexity and relevance, two opposing bills were presented to the British parliament in 1875: the “Henniker bill,” named after its sponsor Lord Henniker and promoted by Frances Cobbe, and the “Playfair bill,” named after scientist and Member of Parliament, Lyon Playfair, and promoted by Charles Darwin himself, along with fellow scientists and friends. Despite coming from opposite ends , both bills proposed reasonable regulation of animal experiments, rather than demanding severe restriction or granting scientists unlimited rights to use animals. Somewhat surprisingly, the Playfair bill drafted by researchers was, in some aspects, more restrictive than Henniker’s by proposing, for instance, that animal experiments should only be performed for the advancement of physiology and not for teaching purposes. The crucial difference was that the Henniker bill called for all researchers and all kinds of experiments to be properly licensed and supervised, as it is today in Great Britain, while the Playfair bill proposed that the law should only be applied to painful experiments. In the absence of parliamentary consensus for either one or the other bill, a Royal Commission—properly balanced to include members of the RSPCA and a few eminent scientists, including T.H. Huxley—was appointed that same year to address this issue, which would result in the 1876 amendment of the 1835 Cruelty to Animals Act in order to regulate the use of animals for scientific purposes, being the first case of this kind of legislation in the world [ 99 , 111 , 117 , 118 ]. This bill would endure for 110 years, until the enactment of the 1986 Animals (Scientific Procedures) Act, and remain the only known legislation to regulate animal experiments for nearly 50 years, despite some attempts to pass similar bills in other Western countries, where antivivisectionism was growing, particularly in Germany, Switzerland, Sweden, and North America [ 14 , 119 ].
The recrudescence and spread of antivivisection feelings in the late nineteenth century was coincidental with the long-awaited beginning of direct clinical and public health benefit from animal research. Before the end of the century, the germ theory of infectious diseases— i.e. , that pathogenic microbes were the causative agent of such diseases, rather than internal causes, “miasmas” in the air or water, or even more esoteric explanations—would gain broad recognition by the medical community, mostly on account of the work of Louis Pasteur (1822–1895) and his German counterpart, Robert Koch (1843–1910), which was largely based on animal experimentation. This knowledge would have an immediate, profound, and enduring effect on public health, surgery and medicine. Although it had been earlier proposed by Ignaz P. Semmelweis (1818–1865) that puerperal fever was caused by infections resulting from poor hygiene of physicians [ 120 ], only after Joseph Lister’s paper On the Antiseptic Principle of the Practice of Surgery (1867)—prompted by Pasteur’s findings—was the importance of hand-washing and instrument sterilization before surgical procedures and child delivery finally acknowledged, leading to a drastic drop in deaths from puerperal fever and post-surgical sepsis. Until then, previous efforts to make hand-washing a standard procedure had been ridiculed by the medical class.
Pasteur, a professor of chemistry with a doctoral thesis on crystallography, would turn his attention to biology in 1848 [ 121 ]. He began by unraveling the biological nature of fermentation (the inhibiting effect of oxygen on fermentation is still called the “Pasteur effect”), moving on to devise solutions of great economic value by tackling wine and beer spoiling, as well as silkworm disease, all of which he properly identified as being caused by microbes. Together with Claude Bernard, a close friend, he would later develop the process of pasteurization to destroy microorganisms in food. Pasteur began hypothesizing that microbes could also be the causative agents of many diseases affecting humans and other animals. Together with his disciples, most notably Emile Roux (1853–1933), he would go on to identify Staphylococcus , Streptococcus , the “septic vibrio” (now Clostridium septicum ), the causative agents of anthrax ( Bacillus anthracis ) and chicken cholera ( Pasteurella multocida ), being the first to develop vaccines for these zoonotic diseases, as well as for Swine Erypselas, thus setting the foundations of modern immunology [ 122 ]. However, it would be Pasteur’s successful use of a therapeutic vaccine against rabies in humans that would grant him international celebrity status [ 107 , 122 , 123 , 124 ].
Pasteur’s work required the experimental infection of numerous animals, as well as inflicting surgical wounds to test antiseptic techniques and disinfectant products, which made him a prime target of antivivisectionists. Either by genuine conviction or pragmatic convenience, amongst the ranks of Pasteur’s critics for his use of animals, one could easily find opponents of vaccination and the germ theory. Pasteur would frequently receive hate letters and threats, mostly for his infection studies on dogs, although he also used chickens, rabbits, rodents, pigs, cows, sheep, and non-human primates ( Figure 4 ). Pasteur was, however, more sensitive to animal suffering than most of his French counterparts. Not only was he uneasy with the experiments conducted—although sure of their necessity—he would also always insist animals be anesthetized whenever possible to prevent unnecessary suffering. He would even use what we now call “humane endpoints” (for a definition, see [ 125 ]): in a detailed description of his method for the prophylactic treatment of rabies (from 1884), the protocol for infecting rabbits with the rabies virus (for ulterior extraction of the spinal cord to produce a vaccine), he stated that: “The rabbit should begin to show symptoms on the sixth or seventh day, and die on the ninth or tenth. Usually the rabbit is not allowed to die, but is chloroformed on the last day in order to avoid terminal infections and unnecessary suffering” [ 126 ]. Furthermore, he would become directly responsible for saving countless animals from the burden of disease and subsequent culling [ 5 , 107 , 113 , 127 , 128 ].

This full-page illustration of Pasteur in his animal facility was published in Harper’s Weekly in the United States, on 21 June 1884. At this time, there was moderate curiosity on Pasteur’s work in the US, which would intensify after his first successful human trials of a therapeutic vaccine for rabies in 1885. In the article, the reader is reassured that the use of dogs is both humane and justified in the interest of mankind. The use of other species, however, is barely mentioned [ 5 ]. Source: Images from the History of Medicine , U.S. National Library of Science.
Robert Koch, a practicing rural physician, would follow the tradition of the great German/Prussian physiologists of his time (and indeed was a student to many of them), providing invaluable contributions to medical knowledge through animal research, mainly in the field of bacteriology and pathology. His famous “Koch postulates” would play an important role in microbiology Along with his associates, Koch developed from scratch methods that are still used today, such as microphotography of organisms, solid medium culture, and staining or microbe quantification. They would go on to identify the causative agents of tuberculosis ( Micobacterium tuberculosis , also known as the “Koch bacillus”), cholera ( Vibrio cholera , albeit 30 years after Filippo Pacini, 1812–1883 [ 129 ]), and anthrax. The overlapping interest of Pasteur and Koch on anthrax would trigger a bitter rivalry between the two, fuelled by their different approaches to microbiology, as well as chauvinistic Germany–France rivalry [ 130 , 131 ]. Koch’s own school of microbiology housed many of the leading late-nineteenth, early-twentieth-century medical researchers. This included Emil von Behring (1854–1917) and Paul Ehrlich (1854–1915), both responsible for the first antitoxin for treatment of diphtheria—developed from horse serum—for which von Behring received the Nobel Prize in 1901. Von Behring would also develop an antitoxin for immunization against tetanus, along with Shibasaburo Kitasato (1853–1931), who had also studied under Koch. In 1908, Ehrlich would also be awarded the Nobel Prize for contributions to immunology, and would yet again be nominated for his contributions to chemotherapy and the development of Salvasaran (an effective treatment against syphilis), in particular [ 132 , 133 , 134 , 135 ]. The development and production of vaccines and antitoxins led to a dramatic increase in the number of animals used in research. The number of animals used by physiologists in the nineteenth century would be negligible in comparison with the several hundred used by Pasteur to develop, test, and produce vaccines, the thousands of mice used by Paul Ehrlich for the production of Salvasaran—his syphilis drug—and the millions of primates that would be used to produce Polio vaccines in the 1950s [ 5 ].
6. The Twentieth-Century Triumph of Science-Based Medicine
By the end of the nineteenth and beginning of the twentieth century, the pharmacopeia had effective, scientifically tested drugs, a landmark that allowed for an increasing number of people to understand the importance and validity of scientifically sound medical knowledge and, with it, the relevance of animal-based research (see [ 113 , 136 , 137 , 138 ]). One could still find as far as the end of the nineteenth century, however, physicians who disregarded the ideals of scientific medicine and vigorously stood by their traditional epistemological view of medicine and clinical practice, which they saw as more of a form of art than as a science. Many such physicians also opposed experiments on live animals and were members of antivivisection societies [ 77 , 139 , 140 , 141 ]. Nonetheless, the medical profession, medicine itself, and human health had now been irreversibly changed by science, and would continue to be pushed forward throughout the twentieth century to now.
The twentieth century would witness astonishing advances in medical knowledge and the treatment of disease. The discovery of vitamins, hormones, antibiotics, safe blood transfusion, new and safer vaccines, insulin, hemodialysis, chemo and radiotherapy for cancer, the eradication of small pox (and the near eradication of poliomyelitis), advanced means of diagnostic and new surgical techniques are but a very few examples of twentieth century’s medical achievements that have not only saved millions of lives—human and non-human—but also allowed countless humans and animals to live a “life worth living,” by the relief of disease-induced suffering. The advances of biomedical research to human health since the dawn of the past century are countless, with animal research playing a role in a number of important discoveries (for an overview, see [ 142 ]). Of the 103 Nobel Prizes in physiology or medicine given since 1901, on 83 occasions work conducted on vertebrate species (other than human) was awarded, while in another four instances, research relied heavily on results obtained from animal experiments in vertebrates conducted by other groups [ 143 ]. Another indirect measure of the impact that biomedical progress had on the twentieth century was the increase in life expectancy, which in some developed countries doubled between 1900 and 2000, and is still on the rise today [ 144 , 145 , 146 ].
By the 1910–1920s, antivivisection groups were fighting an increasingly difficult war for the public’s support. The argument that no medical progress could be obtained through animal research was becoming increasingly difficult to uphold and, as researchers pledged to avoid animal suffering whenever possible, criticism of animal experiments on the grounds of cruelty toned down. However, not all scientists had sufficient, if any, consideration for animal suffering, and research would continue to be unregulated in most countries. Nevertheless, the exaggerated claims, radical abolitionist views, and scientific denialism by more inflexible antivivisectionists would make them lose support from the general public and more moderate animal protection groups, leading to a decline—albeit not an end—to the antivivisection movement, until its resurgence in the 1970s. Confronted with a general lack of support, moreover in a period that would witness two great world wars and a serious economic recession—which would push the interests of animals further to the background—the line of action of antivivisectionists through most of the twentieth century focused on banning the use of dogs and other companion animals [ 5 , 147 , 148 , 149 , 150 ].
The toning down of the opposition to animal use in the life sciences had also something to do with the emergence of rodent species as a recurrent animal model in research. Unlike dogs or horses, rodents like mice and rats were seen as despicable creatures by most of the public, and therefore less worthy of moral consideration, which in turn deemed their use in research more acceptable [ 147 ]. While this came as an advantage to researchers, it is hard to say, however, if the actual weight of the public’s misgivings about the use of domestic animals was a relevant contributing factor for the ready adoption of rodent models, especially when considering their other numerous advantages as experimental animals when compared to other species. Firstly, they are small, easy to handle, and relatively cheap to house. Secondly, they are highly resistant to successive inbreeding and have a short lifespan and rapid reproduction rate [ 151 , 152 ].
Domesticated rats ( Rattus norvegicus ) were the first rodent species to be used for scientific purposes. Their use in physiological research dates to as early as 1828, but only in the first decades of the twentieth century did they become a preferred tool in research, after the development in 1909 of the first standard rat strain, the Wistar Rat , from which half of all rats used in laboratories today are estimated to have descended (for a historical perspective, see [ 153 , 154 ]) ( Figure 5 ). The mouse ( Mus musculus ) had also been used in the nineteenth century, famously by Gregor Mendel in his 1850s studies on heredity of coat color, until the local bishop censored mouse rearing as inappropriate for a priest, which made him turn to using peas instead [ 155 ]. The mouse would be again picked up in the beginning of the nineteenth century by Lucien Cuénot (1866–1951) to demonstrate that mammals also possessed “genes” (a vague concept at the time) that followed the laws of Mendelian inheritance, and would since then become a privileged model in the study of genetics, a field that would grow exponentially after the discovery of the DNA structure in 1953 by James Watson (born 1928) and Francis Crick (1916–2004). In 1980 John Gordon and Franck Ruddle developed the first transgenic mouse [ 156 ], and in 1988, the first gene knockout model was produced, which granted Mario R. Capecchi (born 1937), Martin J. Evans (born 1941), and Oliver Smithies (born 1925) the 2007 Nobel Prize. In 2002, the mouse became the second mammal, after humans, to have its whole genome sequenced. These, along with other technologies, have opened unlimited possibilities for the understanding of gene function and their influence in several genetic and non-genetic diseases, and have made the mouse the most commonly used animal model in our day (for a historical overview of the use of the mouse model in research, see [ 157 , 158 ]), with prospects being that it will continue to have a central role in biomedicine in the foreseeable future.

Two outbred laboratory rats, of the Lister Hooded (Long–Evans) strain. Rodents are the most commonly used laboratory animals, making up nearly 80% of the total of animals used in the European Union, followed by cold-blooded animals (fish, amphibian and reptiles, making up a total of 9.6%) and birds (6.3%) [ 159 ] Photo: Francis Brosseron, reproduced with permission.
7. Animal Liberation and the Pathway for a More Humane Science
Opposition to animal experiments resurged in the second half of the twentieth century, in particular after the 1975 publication of Animal Liberation by Australian philosopher Peter Singer (born 1946) [ 160 ]. Singer offered a strong philosophical grounding for the animal rights movement, by arguing that the use of animals in research—as well as for food, clothing or any other purpose—is mostly based on the principle of speciesism (coined by Richard Ryder in 1970 [ 161 ]), under which animals are attributed a lower moral value on the sole basis of belonging to a different species [ 162 ], which he considers to be no less justifiable than racism or sexism. His argument, however, does not stem from the premise that animals have intrinsic rights. As a preference utilitarian—and unlike hedonistic utilitarians like Bentham and Mill who argued we should act in order to maximize net happiness—Singer proposed that our actions should aim to do what on balance “furthers the interests of those affected” [ 163 ]. Holding that the interest of all sentient beings to both avoid pain and have positive experiences deserves equal consideration, he thus argues that it is difficult to justify animal research, since it generally does not hold to Bentham’s “ Each to count for one and none for more than one ” postulate. Furthermore, it is usually unfeasible to prospectively quantify how many may benefit directly from a given animal experiment. According to Singer, by using the principle of equal consideration of interests, one should give priority to relieving the greater suffering. Singer does not propose we should assume different species suffer similarly under the same conditions but, on the contrary, that care should be taken when comparing the interests of different species as, for instance, a human cancer patient, for his higher cognitive skills, can suffer a great deal more than a mouse with the same disease [ 164 ]. For this reason, he does not consider animal research to always be morally wrong in principle, and even admits that in certain occasions it may be justifiable, albeit these situations are, in his view, exceptional [ 165 ].
The animal rights movement would, however, receive from American philosopher Tom Regan (born 1938) a more uncompromising view of our duties to animals than Singer’s utilitarianism, one that would question the use of animals in research—or in any other way—altogether, regardless of the purpose of research. In Regan’s book The Case for Animal Rights (1983), he proposed we should extend the Kantian concept of intrinsic value to all sentient beings. This perspective inherently affords vertebrates rights, despite their incapacity to understand or demand such rights, as it is also the case—Regan argues—of small infants and the severely mentally handicapped. Hence, the respect for the life and wellbeing of sentient animals should be taken as absolute moral values, which can only be violated in very specific and extreme cases—such as self-defense. Regan’s moral philosophy hence only allows for an abolitionist view on animal research—since no “ends” can justify the “evil means” of sacrificing an animal in the face of the inviolable dignity of sentient beings [ 166 ]—and has become the main theoretical reference for the animal rights movement.
From the impact of Singer’s and Regan’s works in society and the academic world, “animal ethics” would emerge as a whole new field of philosophical and bioethical studies, and, with it, new and diverse ethical views on animals—including on animal research—and of our duties towards them. However, despite the diversity of philosophical views on the use of animals, the public debate on animal research would become polarized between animal rights activists and animal research advocates. While the first would uphold an uncompromising abolitionist stand, one could also find on the opposite side several persons who did not regard animal research as a moral issue at all [ 167 ]. Furthermore, and despite the debate in the philosophical ground remained civilized—even between diametrically opposed perspectives, see, for example, [ 168 ]—in the “real world” the antagonism began to build up. In the 1970s, animal rights extremist groups began resorting to terrorist actions, thus becoming a serious problem for researchers and authorities in several Western countries still today. These actions more often consist of trespassing, raiding animal facilities and laboratories, damage to property, harassment and death threats to researchers, their families and neighbors. It has also sometimes escalated into kidnapping, car and mail bombings, arson of homes and research facilities, mailing of AIDS-contaminated razorblades, and violence against scientists and their family members [ 169 , 170 ]. These actions, which have been classified as unjustifiable and damaging to the animal rights cause by Tom Regan himself [ 171 ], made researchers close themselves within their community and avoid speaking publicly about their work [ 172 , 173 , 174 ], which in turn left pro-research advocacy to emotion-appealing campaigns, of the likes of the Foundation for Biomedical Research’s “Will I be alright, Doctor?” film [ 175 ], or the advertisement depicted in Figure 6 .

A large advertisement published in the 13 May 1991 edition of The Hour (p. 9), and part of a campaign in defense of animal research, sponsored by the United States Surgical Corporation. While the value of Pasteur’s work is undeniable, there is, however, no scientific grounding for the claim that only by experimenting on dogs would a vaccine for rabies have been developed, or that other animal models or even non-animal methods could not have been used to achieve this in over a century. These dramatic and biased portraits of animal research are now more uncommon, as an increasing number of scientists acknowledge the need to be more candid and open to objective discussion over the possibilities and limitations of animal research, and of the scientific process altogether.
In spite of the emergence of the animal rights movement, animal research for biomedical purposes was—as it continues to be—seen as morally acceptable by the majority of the public [ 176 , 177 ]. It became, however, increasingly evident that animal suffering was morally and socially relevant, and that an ethical balance between the benefits brought about by biomedical progress and the due consideration to animal wellbeing should be sought. However, whilst antivivisection movements would only re-emerge in the late 1970s [ 5 , 178 ], the need for a more humane science had already been acknowledged and addressed within the scientific community as early as the 1950s.
Following the first edition of the Universities Federation for Animal Welfare’s Handbook on the Care and Management of Laboratory Animals (1954), the organization’s founder Charles Hume commissioned that same year a general study on humane techniques in animal experimentation to zoologist and classicist (and overall polymath) William Russell (1925–2006) and microbiologist Rex Burch (1926–1996), under a project chaired by immunologist Peter Medawar (1915–1987), Nobel Prize laureate in 1960 [ 179 , 180 , 181 ]. From this work, Russell and Burch would develop the tenet of the “Three Rs”— Replacement, Reduction, Refinement —principles that would be extensively developed in their seminal book, The Principles of Humane Experimental Technique [ 182 ]. In this book, the authors argued “humane science” to be “best science,” going so far as to state that “If we are to use a criterion for choosing experiments to perform, the criterion of humanity is the best we could possibly invent.” Replacement was defined as “any scientific method employing non-sentient material [to] replace methods which use conscious living vertebrates”; Reduction as the lowering of “the number of animals used to obtain information of a given amount and precision”; and Refinement as the set of measures undertaken to “decrease in the incidence or severity of […] procedures applied to those animals which have to be used,” later including also the full optimization of the wellbeing of laboratory animals, also seen as a basic requirement for the quality of science [ 179 ]. They also challenged the commonly held belief that vertebrate animals—and mammals in particular—are always the most suitable models in biomedical research, a reasoning they called the high-fidelity fallacy . Despite receiving a warm welcome, Russell and Burch’s work would remain largely ignored well into the 1970s. In 1978, physiologist David Henry Smyth (1908–1979) would again bring the Three Rs to the light of day and encompass them under the concept of alternatives [ 67 , 183 ], which he defined as “all procedures which can completely replace the need for animal experiments, reduce the numbers of animals required, or diminish the amount of pain or distress suffered by animals in meeting the essential needs of man and other animals” [ 184 ]. More than a restatement of the Three Rs, this definition had the added value of placing onto researchers the burden of providing convincing evidence for the necessity of using animals [ 183 ], a particularly important statement from the then-president of the UK’s Research Defence Society.
The Three Rs approach would provide an ethically and scientifically sound framework on which a reformist approach to the use of animals in biomedicine could be grounded. It would also set the stage for a more moderate advocacy of animal rights to appear: while remaining incompatible with an abolitionist animal rights perspective, this paradigm grants animals something like a right to protection from suffering, or at least certain suffering beyond a defined threshold [ 185 ], preserving the central idea that there are absolute and non-negotiable limits to what can be done to animals. This welfarist perspective stems from a utilitarian view that animals can be used as means to an end as long as their interests—as far as they can be ascertained—are taken into account, but also accepting that the lives and wellbeing of human beings must be granted greater consideration than animals’. Utilitarian philosopher Raymond G. Frey (1925–2012) offered a philosophical view compatible with the current paradigm, by acknowledging that what we do to animals matters morally, since animals’ sentience and ability to control their lives grants them moral standing and a rightful place in the “moral community.” However, when weighing the interests of humans against animals’ interests (or between animals, or humans), he held that the main question should not lie on one who has moral standing or not, or to which degree, but rather on whose life may be more valuable. In Frey’s view, the value of life “is a function of its quality, its quality of its richness, and its richness of its capacities and scope for enrichment.” Hence, as a result of their higher cognitive capabilities, human lives are typically richer than animal lives, being therefore generally more valuable [ 186 ].
A “welfarist–reformist” approach has been accepted as a compromise by some prominent animal rights advocates who, while maintaining the long-term goal of a full end to all animal experiments, believe that it is by successive short-term improvements of the status quo that their goal can be achieved; see [ 178 , 187 , 188 ]. This position—also endorsed by influential animal advocacy groups like the Humane Society of the United States, or the UK’s FRAME—has, however, been highly criticized by less compromising animal rights advocates, like Regan and Gary Francione (born 1954), who believe reformist attitudes validate and perpetuate the exploitation of animals [ 171 , 189 , 190 ].
The 1980s and the 1990s would witness considerable progress in the development and acknowledgment of the Three Rs, to the satisfaction of William Russell and Rex Burch, who lived to see the “rediscovery” of their principles and the emergence of a whole new field of research inspired by their groundbreaking work [ 179 , 191 ]. As Peter Medawar had predicted in the 1960s, the number of animals used in research would peak in the 1970s and start to decline thereafter, although the number of biomedical papers has since then more than doubled [ 181 , 192 , 193 , 194 , 195 , 196 ]. This data is, however, limited to the Western world, as statistics on animal use in emerging countries such as India and China are unavailable [ 197 ], and there is no way to assess if (and, if so, to what extent) the decline in numbers of animals used in Western countries may be attributed to the outsourcing of animal experiments to these emerging countries. In recent years, the rise in the use of genetically modified animals has led to the stabilization of what would otherwise be a continuously downward trend [ 198 , 199 ] ( Figure 7 ).

This schematic illustration (adapted with permission from an original by Professor Bert van Zupthen) attempts to describe trends in the use of animals for scientific purposes in the Western world across time. It depicts the emergence of the first vivisection studies by classical Greek physicians, the absence of animal-based research—along with most medical and scientific research—across the Middle Ages, its resurgence in the Renaissance onwards, and the rapid increase in animal studies following the rise of science-based physiology and medicine in the nineteenth century. The curves represented are nevertheless conjectural, as there are no reliable statistics on animal use for most of the period covered. Even nowadays it is hard to estimate trends in animal research, as data from several developed countries is insufficient (for instance, in the United States, rodents, fish and birds are not accounted for in the statistics). The available data, however, suggest that the number of animals used in research and testing in the Western world peaked in the 1970s, and decreased until the late 1990s, or early 2000s, to about half the number of 30 years earlier, and stabilizing in recent years. While many, if not most, researchers do not foresee an end to animal experiments in biomedicine, the European Commission has nevertheless set full replacement of animal experiments as an ultimate goal [ 204 ], and the Humane Society of the United States has the optimistic goal of full replacement by the year 2050 [ 192 ].
In 1999, the Declaration of Bologna, signed in the 3rd World Congress on Alternatives and Animal Use in the Life Sciences, would reaffirm that “ humane science is a prerequisite for good science, and is best achieved in relation to laboratory animal procedures by the vigorous promotion and application of the Three Rs ” [ 200 ]. The Three Rs would also become the overarching principle of several legislative documents regulating animal use in science since the 1980s (including the latest European legislation [ 201 ]). Most recently, biomedical researchers in both industry and academia have also acknowledged the central importance of the Three Rs and the need for more transparency regarding animal use in biomedical research through the Basel Declaration [ 202 , 203 ]. More important, there are currently thousands of scientists devoted to the progress of animal welfare and development of alternatives to animal use in the life sciences.
8. Conclusion
The historical controversy surrounding animal research is far from being settled. While the key arguments in this debate have not differed significantly since the rise of antivivisectionism in nineteenth-century England—and even before—we have since then moved a long way forward in regards to the protection of animals used in research and transparency regarding such use. While animal experiments have played a vital role in scientific and biomedical progress and are likely to continue to do so in the foreseeable future, it is nonetheless important to keep focusing on the continuous improvement of the wellbeing of laboratory animals, as well as further development of replacement alternatives for animal experiments.
Acknowledgments
The author thanks Francis Brosseron ( Lycée Français du Porto ) for the photograph in Figure 5 , Bert van Zutphen (Emeritus Professor, Utrecht University) for the original picture that has been adapted for Figure 7 , and I. Anna S. Olsson, Manuel Sant’Ana (IBMC, University of Porto) and four anonymous referees for their valuable comments on this manuscript.
Conflict of Interest
The author declares no conflict of interest.
References and Notes
We use cookies to understand how you use our site and to improve your experience. This includes personalizing content and advertising. To learn more, click here . By continuing to use our site, you accept our use of cookies, revised Privacy Policy and Terms of Service .
New to Zacks? Get started here.
Member Sign In
Don't Know Your Password?
- Zacks #1 Rank
- Zacks Industry Rank
- Zacks Sector Rank
- Equity Research
- Mutual Funds
- Mutual Fund Screener
- ETF Screener
- Earnings Calendar
- Earnings Releases
- Earnings ESP
- Earnings ESP Filter
- Stock Screener
- Premium Screens
- Basic Screens
- Research Wizard
- Personal Finance
- Money Managing
- Real Estate
- Retirement Planning
- Tax Information
- My Portfolio
- Create Portfolio
- Style Scores
- Testimonials
- Zacks.com Tutorial
Services Overview
- Zacks Ultimate
- Zacks Investor Collection
- Zacks Premium
Investor Services
- ETF Investor
- Home Run Investor
- Income Investor
- Stocks Under $10
- Value Investor
- Top 10 Stocks
Other Services
- Method for Trading
- Zacks Confidential
Trading Services
- Black Box Trader
- Counterstrike
- Headline Trader
- Insider Trader
- Large-Cap Trader
- Options Trader
- Short Sell List
- Surprise Trader
- Alternative Energy
You are being directed to ZacksTrade, a division of LBMZ Securities and licensed broker-dealer. ZacksTrade and Zacks.com are separate companies. The web link between the two companies is not a solicitation or offer to invest in a particular security or type of security. ZacksTrade does not endorse or adopt any particular investment strategy, any analyst opinion/rating/report or any approach to evaluating individual securities.
If you wish to go to ZacksTrade, click OK . If you do not, click Cancel.
Image: Bigstock
3 Medical Device Stocks With Solid Dividend Yield: CAH & Others
The Zacks Medical sector is facing headwinds in the form of inflation, higher interest rates, supply-chain disruptions and high operating costs. These factors are likely to put pressure on the industry players’ margin.
Amid these ongoing headwinds, the sector has gained 2.5% until Apr 9, underperforming the S&P 500 Index’s 9.4% gain.
Meanwhile, amid the rising risk of a downtrend in the market, it would be a wise decision to invest in some dividend-paying companies like Cardinal Health ( CAH Quick Quote CAH - Free Report ) , Baxter International ( BAX Quick Quote BAX - Free Report ) and Fresenius Medical Care ( FMS Quick Quote FMS - Free Report ) from the medical device industries to create a steady income source. These companies have consistently announced dividend hikes, thereby highlighting their pro-shareholder stance.
Stocks with a strong history of dividend growth are mature and less susceptible to large swings in the market. They act as a hedge against economic or political uncertainty as well as stock market volatility. At the same time, the stocks also offer downside protection with a consistent rise in payouts.
Additionally, these companies have superior fundamentals like a sustainable business model, a long track of profitability, rising cash flows, good liquidity, a strong balance sheet and some value characteristics.
3 Medical Products Stocks to Embrace Now
In order to choose some of the best dividend stocks from the industry, we have run the Zacks Stock Screener to identify those with a dividend yield in excess of 1.5% and a sustainable dividend payout ratio of less than 50%.
Cardinal Health: Headquartered in Dublin, OH, Cardinal Health is a nationwide drug distributor and provider of services to pharmacies, healthcare providers and manufacturers. The company pays out a quarterly dividend of 50 cents ($2.00 annualized) per share, which gives it a 1.85% yield at the current stock price. This company’s payout ratio is 29%, with a five-year dividend growth rate of 0.96%. ( Check Cardinal’s dividend history here .)
The company is also active on the buyback front. During the six months ended Dec 31, 2023, it deployed $750 million for share repurchases and $255 million for cash dividends. As of December-end, it had $3.5 billion available under the share repurchase program, previously authorized by the board of directors.
Baxter International: Headquartered in Deerfield, IL, Baxter engages in the development, manufacture and sale of a broad range of products, digital health solutions and therapies used by hospitals and other care-giving organizations, including at-home physicians.
Baxter pays annualized dividends of $1.16 per share, resulting in a 2.71% yield at the current stock price. This company’s payout ratio is 43%, with a five-year dividend growth rate of 7.2%. ( Check Baxter’s dividend history here .)
The company also has buyback plans. Although it did not repurchase shares during the fourth quarter of 2023, it had $1.3 billion under its share repurchase authorization as of December 2023. BAX had repurchased 500,000 shares in 2022.
Fresenius Medical Care: Headquartered in Germany, Fresenius Medical is one of the largest integrated providers of products and services for individuals undergoing dialysis following chronic kidney failure. FMS pays out an annual dividend of 42 cents per share, which gives it a 2.16% yield at the current stock price. This company’s payout ratio is 30%. ( Check Fresenius Medical’s dividend history here .)
Unique Zacks Analysis of Your Chosen Ticker
Pick one free report - opportunity may be withdrawn at any time.
Baxter International Inc. (BAX) - $25 value - yours FREE >>
Cardinal Health, Inc. (CAH) - $25 value - yours FREE >>
Fresenius Medical Care AG & Co. KGaA (FMS) - $25 value - yours FREE >>
Published in
This file is used for Yahoo remarketing pixel add
Due to inactivity, you will be signed out in approximately:
Help | Advanced Search
Computer Science > Computation and Language
Title: medical mt5: an open-source multilingual text-to-text llm for the medical domain.
Abstract: Research on language technology for the development of medical applications is currently a hot topic in Natural Language Understanding and Generation. Thus, a number of large language models (LLMs) have recently been adapted to the medical domain, so that they can be used as a tool for mediating in human-AI interaction. While these LLMs display competitive performance on automated medical texts benchmarks, they have been pre-trained and evaluated with a focus on a single language (English mostly). This is particularly true of text-to-text models, which typically require large amounts of domain-specific pre-training data, often not easily accessible for many languages. In this paper, we address these shortcomings by compiling, to the best of our knowledge, the largest multilingual corpus for the medical domain in four languages, namely English, French, Italian and Spanish. This new corpus has been used to train Medical mT5, the first open-source text-to-text multilingual model for the medical domain. Additionally, we present two new evaluation benchmarks for all four languages with the aim of facilitating multilingual research in this domain. A comprehensive evaluation shows that Medical mT5 outperforms both encoders and similarly sized text-to-text models for the Spanish, French, and Italian benchmarks, while being competitive with current state-of-the-art LLMs in English.
Submission history
Access paper:.
- HTML (experimental)
- Other Formats
References & Citations
- Google Scholar
- Semantic Scholar
BibTeX formatted citation
Bibliographic and Citation Tools
Code, data and media associated with this article, recommenders and search tools.
- Institution
arXivLabs: experimental projects with community collaborators
arXivLabs is a framework that allows collaborators to develop and share new arXiv features directly on our website.
Both individuals and organizations that work with arXivLabs have embraced and accepted our values of openness, community, excellence, and user data privacy. arXiv is committed to these values and only works with partners that adhere to them.
Have an idea for a project that will add value for arXiv's community? Learn more about arXivLabs .
IMAGES
VIDEO
COMMENTS
The evolution of clinical research traverses a long and fascinating journey. The recorded history of clinical trials goes back to the biblical descriptions in 500 BC. The journey moves from dietary therapy - legumes and lemons - to drugs. After basic approach of clinical trial was described in 18th century, the efforts were made to refine ...
The University of Florida Cancer and Genetics Research Complex is an integrated medical research facility. Medical research (or biomedical research ), also known as health research, refers to the process of using scientific methods with the aim to produce knowledge about human diseases, the prevention and treatment of illness, and the promotion ...
Dana-Farber researchers clone the gene ras and demonstrate that, when mutated, this gene—the first known human oncogene—helps spur the development of many common human tumors.; Mass General researchers pioneer the positron emission tomography (PET) scan, an imaging technique that made possible one of the first noninvasive looks at functional changes within the brain and other organs.
The ancient Middle East and Egypt. The establishment of the calendar and the invention of writing marked the dawn of recorded history. The clues to early knowledge are few, consisting only of clay tablets bearing cuneiform signs and seals that were used by physicians of ancient Mesopotamia.In the Louvre Museum in France, a stone pillar is preserved on which is inscribed the Code of Hammurabi ...
The Nuremberg Code is the most important document in the history of the ethics of medical research. 1-6 The Code was formulated 50 years ago, in August 1947, in Nuremberg, Germany, by American ...
Clinical trials are under way around the world, including in Australia, testing COVID-19 vaccines and treatments. These clinical trials largely fall into two groups. With observational studies ...
Abstract. The Oxford Handbook of the History of Medicine celebrates the richness and variety of medical history around the world. In recent decades, the history of medicine has emerged as a rich and mature sub-discipline within history, but the strength of the field has not precluded vigorous debates about methods, themes, and sources.
Visit the Research Tools; New Exhibition. Take Two and Call Me in the Morning: The Story of Aspirin Revisited. ... Press Play. Explore 100 years of motion picture medical history on YouTube at NLM. NLM Collections on Instagram. Visit @nlm_collections highlighting the collections of the world's largest biomedical library. Previous Next ...
Abstract. The evolution of clinical research traverses a long and fascinating journey. From the first recorded trial of legumes in biblical times to the first randomized controlled of trial of streptomycin in 1946, the history of clinical trial covers a wide variety of challenges - scientific, ethical and regulatory.
History of Medicine Timeline. 2600 BC The Egyptian Imhotep describes the diagnosis and treatment of 200 diseases. 500 BC Alcmaeon of Croton distinguished veins from arteries. 460 BC Birth of Hippocrates, the Greek father of medicine begins the scientific study of medicine and prescribes a form of aspirin. 300 BC Diocles wrote the first known ...
It contains material dated from the 1400s through 1950 and is an important resource for researchers in the history of medicine, history of science, and for clinical research. NLM has scanned all 61 volumes of the printed Index-Catalogue and made them available in NLM Digital Collections grouped by series: Series 1 , Series 2 , Series 3 , Series ...
A research collection covering all aspects of the history of medicine, public health and allied sciences, it contains over 70,000 volumes. A large, comprehensive library of secondary sources accompanies a smaller, but choice collection of rare books, manuscripts, prints, photographs, medals, stamps and objects.
The Bulletin publishes scholarly articles spanning the social, cultural, and scientific aspects of the history of medicine worldwide.Articles are based on historical research in primary sources grounded in the robust secondary literature in the history of medicine. Article submissions should clearly make critical interpretations and place the story in historical context.
The Human Genome Project (HGP) was a collaborative scientific research program on international scale conducted to discover all the chemical base pairs which make up human DNA for further biological studies. Its primary goal was to map and identify both physically and functionally, the approximately 20,000-25,000 genes of the human genome.
In planning for the commemoration of the NIH's centennial in 1987, Dr. DeWitt Stetten Jr., proposed the establishment of a museum of medical research to preserve the material heritage of the NIH. Stetten had first come to the NIH in 1954 as director of the intramural research program of the National Institute of Arthritis and Metabolic Diseases ...
The DeWitt Stetten Jr. Museum of Medical Research, established in 1986, preserves and interprets the material culture of the scientific work of the NIH. In conjunction with the broader Office of NIH History, the Stetten Museum collects biomedical research instruments, photographs, videos, journals, oral histories, and objects related to the ...
Human challenge trials are as old as inoculation itself. In 1796, English surgeon Edward Jenner tested the world's first vaccine by exposing his gardener's 8-year-old son to cowpox and then ...
The Stanford University Medical Experimental-Artificial Intelligence in Medicine, a time-shared computer system, was created in 1973 and enhanced networking capabilities among clinical and biomedical researchers from several institutions. 12 Largely as a result of these collaborations, the first National Institutes of Health-sponsored AIM ...
History & Mission. The Stowers Institute is a place where scientists can openly pursue and discover the secrets of life. Thanks to the vision of our founders and our unique funding model, we can transform science, allowing the opportunity to expand and accelerate our understanding of human health and disease. The Stowers Institute is a place ...
Researchers, doctors and participants gathered in Framingham on Monday to celebrate the 75th anniversary of the monumental research study, now the longest running cohort study in the history of ...
Scientists face challenges in communicating about their careers in biomedical research to the public, despite the importance of doing so. Here, we discuss tools and resources for outreach, such as posters, videos, and presentations that can be leveraged by scientists to help educate communities about the pivotal role of animals in medical progress.
Background: Medical history contributes approximately 80% to the diagnosis, although physical examinations and laboratory investigations increase a physician's confidence in the medical diagnosis. The concept of artificial intelligence (AI) was first proposed more than 70 years ago. Recently, its role in various fields of medicine has grown remarkably.
Abstract. The use of non-human animals in biomedical research has given important contributions to the medical progress achieved in our day, but it has also been a cause of heated public, scientific and philosophical discussion for hundreds of years. This review, with a mainly European outlook, addresses the history of animal use in biomedical ...
Here we discuss three medical device stocks, Cardinal Health (CAH), Baxter International (BAX) and Fresenius Medical Care (FMS), with a solid five-year dividend growth history.
Research on language technology for the development of medical applications is currently a hot topic in Natural Language Understanding and Generation. Thus, a number of large language models (LLMs) have recently been adapted to the medical domain, so that they can be used as a tool for mediating in human-AI interaction. While these LLMs display competitive performance on automated medical ...