
An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Med Sci Educ
- v.31(1); 2021 Feb

Teaching Critical Thinking and Problem-Solving Skills to Healthcare Professionals
Jessica a. chacon.
Department of Medical Education, Paul L Foster School of Medicine, Texas Tech University Health Sciences Center El Paso, El Paso, TX USA
Herb Janssen
Associated data, introduction.
Determining approaches that improve student learning is far more beneficial than determining what can improve a professor’s teaching. As previously stated, “Lecturing is that mysterious process by which the contents of the note-book of the professor are transferred through the instrumentation of the fountain-pen to the note-book of the student without passing through the mind of either” [ 1 ]. This process continues today, except that the professor’s note-book has been replaced with a PowerPoint lecture and the student’s note-book is now a computer.
In 1910, the Flexner report noted that didactic lectures were antiquated and should be left to a time when “professors knew and students learned” [ 2 ]. Approximately 100 years later, the Liaison Committee on Medical Education (LCME) affirmed Flexner’s comment and suggested that student learning must involve active components [ 3 ]: It seems somewhat obscured that almost 100 years separated these two statements.
Our strategy requires the following: student engagement in the learning process; a curriculum that develops a foundation for each student’s knowledge acquisition; focusing primarily on student learning instead of professor teaching; helping enable students develop critical thinking skills; and encouraging students to develop “expertise” in their chosen discipline.
Six fundamental topics that play a role in the development of a health sciences student’s critical thinking ability will be described. In “Section I,” these topics will be discussed independently, highlighting the importance of each. In “Section II: Proposed Curriculum and Pedagogy to Improve Student Learning,” the topics will be united into a practical approach that can be used to improve student learning, curriculum, pedagogy, and assessment.
Foundation Knowledge
Students use mnemonics to provide a foundation for new information. Although mnemonics help students associate information that they want to remember with something they already know, students learn tads of information that is not placed into a practical, meaningful framework developed by the student [ 4 , 5 ]. This commentary highlights the problem of recalling facts when these facts are presented in isolation. The responsibility for this resides not with the student, but with a curriculum that teaches isolated facts, instead of integrated concepts.
A taxonomy for significant learning presented by Dr. Fink emphasizes the need to develop foundational knowledge before additional information can be learned in an effective manner [ 6 ]. He provides suggestions on developing specific learning goals in given courses. Two of his most important criteria are (1) the development of a foundation of knowledge and (2) helping students “learn how to learn” [ 6 ].
Learning Approaches and Abilities
Howard Gardner introduced the concept of multiple intelligences in the 1980s [ 7 ]. Gardner expanded this idea to include intelligence in the areas of (1) Verbal-linguistic, (2) Logical-mathematical, (3) Spatial-visual, (4) Bodily-kinesthetic, (5) Musical, (6) Interpersonal, (7) Intrapersonal personal, (8) Naturalist, and (9) Existential. He concluded that students gifted in certain areas will be drawn in that direction due to the ease with which they excel. While it is important to recognize these differences, it is crucial to not ignore the need for student development in areas where they are less gifted. For example, students gifted in mathematics who fail to develop intrapersonal and interpersonal skills will more likely become recluse, limiting their success in real-world situations [ 7 , 8 ]. Similar examples can also be found in the medical world [ 7 , 8 ].
Based on Gardner’s work, it seems evident that students admitted to our health sciences schools will arrive with different skills and abilities. Despite this, educators are required to produce graduates who have mastered the competencies required by the various accrediting agencies. Accomplishing this task demands sensitivity to the students’ different abilities. While the curriculum remains focused on the competencies students must demonstrate when training is complete. Creating this transition using a traditional lecture format is difficult, if not impossible.
Active Engagement
In 1910, Flexner suggested that didactic lecture is important; however, it should be limited only to the introduction or conclusion of a given topic [ 2 ]. Flexner stated that students should be given the opportunity to experience learning in a context that allowed them to use scientific principles rather than empirical observations [ 2 ]. Active engagement of the student in their learning process has been recently promoted by the LCME [ 3 ]. This reaffirmation of Flexner’s 1910 report highlights the incredibly slow pace at which education changes.
Critical Thinking
Critical thinking is an active process that, when applied appropriately, allows each of us to evaluate our own activities and achievements. Critical thinking also allows an individual to make minor, mid-course corrections in thinking, instead of waiting until disastrous outcomes are unavoidable.
Educators in Allied Health and Nursing have included critical thinking as part of their curriculum for many years [ 9 ]. Medical educators, on the other hand, have not fully integrated critical thinking as part of their curriculum [ 10 , 11 ].
Bloom’s taxonomy has often been used to define curriculum [ 12 ]. The usefulness and importance of Bloom’s taxonomy is not to be underestimated; however, its limitations must also be addressed. As Bloom and his colleagues clearly stated, their taxonomy describes behavioral outcomes and is incapable of determining the logical steps through which this behavior was developed [ 12 ]. Bloom highlights this shortcoming in his initial book on the cognitive domain. He described two students who solved the same algebra problem. One student does this by rote memory, having been exposed to the problem previously, while the other student accomplishes the task by applying mathematical principles. The observer has no way of knowing which approach was used unless they have prior knowledge of the students’ background [ 12 ]. The importance of this distinction becomes apparent in medical problem-solving.
Contextual Learning
Enabling students to learn in context is critical; however, trying to teach everything in context results in a double-edged sword [ 13 ]. On the one hand, learning material in context helps the student develop a solid foundation in which the new information can be built. On the other hand, the educator will find it impossible to duplicate all situations the student will encounter throughout his or her career as a healthcare provider. This dilemma again challenges the educator to develop a variety of learning situations that simulate real-world situations. It seems that “in context” can at best be developed by presenting a variety of patients in a variety of different situations.
In the clinical setting, the physician cannot use a strict hypothesis-driven study on each patient, but must treat patients using the best, most logical treatment selected based on his or her knowledge and the most reliable information.
Development of Expertise
Several researchers have studied the characteristics required of expert performance, the time required to obtain these traits, and the steps that are followed as an individual’s performance progresses from novice to expert.
Studies involving expert physicians have provided data that can be directly used in our attempt to improve curriculum and pedagogy in the healthcare profession. Patel demonstrated that medical students and entry-level residents can recall a considerable amount of non-relevant data while the expert cannot [ 14 ]. Conversely, the expert physician has a much higher level of relevant recall, suggesting they have omitted the non-relevant information and retained only relevant information that is useful in their practice. Using these methods, the expert physicians produce accurate diagnosis in almost 100% of cases, while the medical students can achieve only patricianly correct or component diagnosis only [ 14 ].
In the healthcare setting, both methods are used. The expert physicians will use forward reasoning when the accuracy of the data allows this rapid problem-solving method. When the patient’s conditions cannot be accurately described using known information, the expert diagnostician will resort to the slower hypothesis-driven, backward reasoning approach. In this manner, the highest probability of achieving an accurate diagnosis in the shortest time will be realized [ 14 ].
Section II: Proposed Curriculum and Pedagogy to Improve Student Learning
The following section will outline several distinct but interrelated approaches to accomplish the six educational principles discussed above. The topics will be highlighted as they apply to the specific topic and each section will be comprised of curriculum, pedagogy, and assessment.
Developing a Knowledge Base Using Active Learning Sensitive to Students’ Abilities
Students admitted into healthcare training programs come from various backgrounds. This is both a strength for the program and a challenge for the educator. The strength is recognized in the diversity the varied backgrounds bring to the class and ultimately the profession. The challenge for the educator is attempting to provide each student with the material and a learning approach that will fit their individual ability and knowledge level. The educator can provide prerequisite objectives that identify the basic knowledge required before the student attempts the more advanced curriculum. Scaffolding questions can also be provided that allow students to determine their mastery of these prerequisite objectives. Briefly, scaffolding questions are categorized based on complexity. Simple, factual questions are identified with a subscript “0” (i.e. 1. 0 , 2. 0 , etc.). Advanced questions have a subscript suggesting the estimated number of basic concepts that must be included/combined to derive the answer.
Using technology to provide these individual learning opportunities online allows each student to address his or her own potential deficits. Obviously, those who find their knowledge lacking will need to spend additional time learning this information; however, using technology, this can be accomplished without requiring additional class time. This approach will decrease learning gaps for students, while excluding unnecessarily repeating material known by others.
The curriculum is divided into two parts: (1) content and (2) critical thinking/problem-solving skills. The basic knowledge and factual content can be provided online. Students are expected to learn this by actively engaging the material during independent study. This saves classroom or small-group sessions for interaction where students can actively learn critical thinking/problem-solving skills.
The curriculum should be designed so that students can start at their own level of understanding. The more advanced students can identify the level appropriate for themselves and/or review the more rudimentary information as needed. As shown by previous investigators, experts omit non-relevant information so that they can focus on appropriate problem-solving. Requiring students to learn by solving problems or exploring case studies will be emphasized when possible.
Technology can be used to deliver the “content” portion of the curriculum. Voice-over PowerPoints and/or video clips made available online through WebCT or PodCast will allow each student to study separately or in groups at their own rate, starting at their own level of knowledge. The content delivered in this fashion will complement the handout and/or textbook information recommended to the students. This will provide the needed basic information that will be used as a foundation for the development of critical thinking and problem-solving. The flipped classroom and/or team-based learning can both be used to help facilitate this type of learning. [ 15 ]
Student Assessments
It is imperative for students to know whether they have mastered the material to the extent needed. This can be accomplished by providing online formative evaluations. These will not be used to determine student performance; however, the results will be provided to the educator to determine the class’s progress and evaluation of the curriculum.
Developing Critical Thinking Skills in the Classroom or Small-Group Setting
Critical thinking skills are essential to the development of well-trained healthcare professionals. These skills are not “taught” but must be “learned” by the student. The educator provides learning experiences through which the students can gain the needed skills and experience. Mastery of the content should be a responsibility placed on the student. Information and assistance are given to the students, but students are held accountable for learning the content. This does not indicate that the educator is freed from responsibility. In fact, the educator will most likely spend more time planning and preparing, compared to when didactic lectures were given; however, the spotlight will be placed on the student. Once the learning modules are developed, they can be readily updated, allowing the educators to improve their sessions with each evaluation.
Curriculum designed to help student students develop critical thinking/problem-solving skills should be learned in context. During the introductory portions of the training, this can be accomplished by providing problem-based scenarios similar to what will be expected in the later clinical setting. The transition to competency-based evaluation in many disciplines has made this a virtual necessity. Critical thinking/problem-solving skills should emphasize self-examination. It should teach an individual to accomplish this using a series of steps that progress in a logical fashion, stressing that critical thinking is a progression of logical thought, not an unguided process.
The methods of teaching critical thinking can be traced back to the dialectic methods used by Socrates. Helping the students learn by posing questions remains an effective tool. Accomplishing this in a group setting also provides each student with the opportunity to learn, not only from their mistakes and accomplishments, but from the mistakes and accomplishments of others. Scenario questions can be presented in a manner similar to those found in many board and licensure exams. This exposes students to material in a format relevant to the clinical setting and to future exams. In larger groups, PowerPoint presentation of scenario questions can be used. Team-based learning (TBL) is useful in encouraging individual self-assessment and peer-peer instruction, while also providing an opportunity for the development of critical thinking and problem-solving skills. After the Individual Readiness Assurance Test (iRAT) exam, students work together to answer the Group Readiness Assurance Test (gRAT). Following this, relevant material is covered by clinicians and basic scientists working together and questions asked using an audience response system. This has been useful in encouraging individual self-assessment and peer-peer instruction while also providing an opportunity for the development of critical thinking and problem-solving skills.
Formative assessment of the students will be given in the class session. This can be accomplished using an audience response system. This gives each individual a chance to determine their own critical thinking skill level. It will prevent the “Oh, I knew that” response from students who are in denial of their own inabilities. Summative assessment in the class will be based on the critical thinking skills presented in the classroom or small-group setting. As mentioned earlier, the students will be evaluated on their ability to think critically and to problem-solve. This will by necessity include evaluation of content knowledge—but only as it pertains to the critical thinking and problem-solving skills. This will be made clear through the use of objectives that describe both content and critical thinking.
Enhancing Critical Thinking Skills in Simulation Centers and Clinics
The development of critical thinking skills in healthcare is somewhat unique. In chess, students can start playing using the same tools employed by the experts (the chess board); however, in healthcare, allowing students to make medical decisions is ethically inappropriate and irresponsible. Simulations centers allow students to gain needed experience and confidence without placing patients at risk. Once the students have mastered simulation center experiences and acquired the needed confidence, they can participate in patient diagnosis under the watchful eye of the expert healthcare professional.
The student’s curriculum now becomes the entire knowledge base of each healthcare discipline. This includes textbooks and journal articles. Students are required to come well prepared to the clinics and/or hospital having developed and in-depth understanding of each patient in their care.
Each day, the expert healthcare provider, serving as a mentor, will provide formative evaluation of the student and his/her performance. Mentors will guide the student, suggesting changes in the skills needed to evaluate the patients properly. In addition, standardized patients provide an excellent method of student/resident evaluation.
Summative evaluation is in the form of subject/board exams. These test the student’s or resident’s ability to accurately describe and evaluate the patient. The objective structured clinical examination (OSCE) is used to evaluate the student’s ability to correctly assess the patient’s condition. Thinking aloud had been previously shown as an effective tool for evaluating expert performance in such settings [ 16 ]. Briefly, think aloud strategies require the student to explain verbally the logic they are using to combine facts to arrive at correct answers. This approach helps the evaluator to determine both the accuracy of the answer and if the correct thought process was followed by the student.
If the time required to develop an expert is a minimum of ten years, what influence can education have on the process?
Education can:
- Provide the student with a foundation of knowledge required for the development of future knowledge and skills.
- Introduce the student to critical thinking and problem-solving techniques.
- Require the student to actively engage the material instead of attempting to learn using rote memory only.
- Assess the performance of the student in a formative manner, allowing the lack of information of skills to be identified early, thus reducing the risk of failure when changes in study skills are more difficult and/or occur too late to help.
- Provide learning in a contextual format that makes the information meaningful and easier to remember.
- Provide training in forward reasoning and backward reasoning skills. It can relate these skills to the problem-solving techniques in healthcare.
- Help students develop the qualities of an expert healthcare provider.
Authors’ Contributions
The authors wrote and contributed to the final manuscript.
Data Availability
Compliance with ethical standards.
The authors declare that they have no conflict of interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
- Type 2 Diabetes
- Heart Disease
- Digestive Health
- Multiple Sclerosis
- COVID-19 Vaccines
- Occupational Therapy
- Healthy Aging
- Health Insurance
- Public Health
- Patient Rights
- Caregivers & Loved Ones
- End of Life Concerns
- Health News
- Thyroid Test Analyzer
- Doctor Discussion Guides
- Hemoglobin A1c Test Analyzer
- Lipid Test Analyzer
- Complete Blood Count (CBC) Analyzer
- What to Buy
- Editorial Process
- Meet Our Medical Expert Board
Medicare Assignment: Everything You Need to Know
Medicare assignment.
- Providers Accepting Assignment
- Providers Who Do Not
- Billing Options
- Assignment of Benefits
- How to Choose
Frequently Asked Questions
Medicare assignment is an agreement between Medicare and medical providers (doctors, hospitals, medical equipment suppliers, etc.) in which the provider agrees to accept Medicare’s fee schedule as payment in full when Medicare patients are treated.
This article will explain how Medicare assignment works, and what you need to know in order to ensure that you won’t receive unexpected bills.
fizkes / Getty Images
There are 35 million Americans who have Original Medicare. Medicare is a federal program and most medical providers throughout the country accept assignment with Medicare. As a result, these enrollees have a lot more options for medical providers than most of the rest of the population.
They can see any provider who accepts assignment, anywhere in the country. They can be assured that they will only have to pay their expected Medicare cost-sharing (deductible and coinsurance, some or all of which may be paid by a Medigap plan , Medicaid, or supplemental coverage provided by an employer or former employer).
It’s important to note here that the rules are different for the 29 million Americans who have Medicare Advantage plans. These beneficiaries cannot simply use any medical provider who accepts Medicare assignment.
Instead, each Medicare Advantage plan has its own network of providers —much like the health insurance plans that many Americans are accustomed to obtaining from employers or purchasing in the exchange/marketplace .
A provider who accepts assignment with Medicare may or may not be in-network with some or all of the Medicare Advantage plans that offer coverage in a given area. Some Medicare Advantage plans— health maintenance organizations (HMOs) , in particular—will only cover an enrollee’s claims if they use providers who are in the plan's network.
Other Medicare Advantage plans— preferred provider organizations (PPOs) , in particular—will cover out-of-network care but the enrollee will pay more than they would have paid had they seen an in-network provider.
Original Medicare
The bottom line is that Medicare assignment only determines provider accessibility and costs for people who have Original Medicare. People with Medicare Advantage need to understand their own plan’s provider network and coverage rules.
When discussing Medicare assignment and access to providers in this article, keep in mind that it is referring to people who have Original Medicare.
How to Make Sure Your Provider Accepts Assignment
Most doctors, hospitals, and other medical providers in the United States do accept Medicare assignment.
Provider Participation Stats
According to the Centers for Medicare and Medicaid Services, 98% of providers participate in Medicare, which means they accept assignment.
You can ask the provider directly about their participation with Medicare. But Medicare also has a tool that you can use to find participating doctors, hospitals, home health care services, and other providers.
There’s a filter on that tool labeled “Medicare-approved payment.” If you turn on that filter, you will only see providers who accept Medicare assignment. Under each provider’s information, it will say “Charges the Medicare-approved amount (so you pay less out-of-pocket).”
What If Your Provider Doesn’t Accept Assignment?
If your medical provider or equipment supplier doesn’t accept assignment, it means they haven’t agreed to accept Medicare’s approved amounts as payment in full for all of the services.
These providers can still choose to accept assignment on a case-by-case basis. But because they haven’t agreed to accept Medicare assignment for all services, they are considered nonparticipating providers.
Note that "nonparticipating" does not mean that a provider has opted out of Medicare altogether. Medicare will still pay claims for services received from a nonparticipating provider (i.e., one who does not accept Medicare assignment), whereas Medicare does not cover any of the cost of services obtained from a provider who has officially opted out of Medicare.
If a Medicare beneficiary uses a provider who has opted out of Medicare, that person will pay the provider directly and Medicare will not be involved in any way.
Physicians Who Have Opted Out
Only about 1% of all non-pediatric physicians have opted out of Medicare.
For providers who have not opted out of Medicare but who also don’t accept assignment, Medicare will still pay nearly as much as it would have paid if you had used a provider who accepts assignment. Here’s how it works:
- Medicare will pay the provider 95% of the amount they would pay if the provider accepted assignment.
- The provider can charge the person receiving care more than the Medicare-approved amount, but only up to 15% more (some states limit this further). This extra amount, which the patient has to pay out-of-pocket, is known as the limiting charge . But the 15% cap does not apply to medical equipment suppliers; if they do not accept assignment with Medicare, there is no limit on how much they can charge the person receiving care. This is why it’s particularly important to make sure that the supplier accepts Medicare assignment if you need medical equipment.
- The nonparticipating provider may require the person receiving care to pay the entire bill up front and seek reimbursement from Medicare (using Form CMS 1490-S ). Alternatively, they may submit a claim to Medicare on behalf of the person receiving care (using Form CMS-1500 ).
- A nonparticipating provider can choose to accept assignment on a case-by-case basis. They can indicate this on Form CMS-1500 in box 27. The vast majority of nonparticipating providers who bill Medicare choose to accept assignment for the claim being billed.
- Nonparticipating providers do not have to bill your Medigap plan on your behalf.
Billing Options for Providers Who Accept Medicare
When a medical provider accepts assignment with Medicare, part of the agreement is that they will submit bills to Medicare on behalf of the person receiving care. So if you only see providers who accept assignment, you will never need to submit your own bills to Medicare for reimbursement.
If you have a Medigap plan that supplements your Original Medicare coverage, you should present the Medigap coverage information to the provider at the time of service. Medicare will forward the claim information to your Medigap insurer, reducing administrative work on your part.
Depending on the Medigap plan you have, the services that you receive, and the amount you’ve already spent in out-of-pocket costs, the Medigap plan may pay some or all of the out-of-pocket costs that you would otherwise have after Medicare pays its share.
(Note that if you have a type of Medigap plan called Medicare SELECT, you will have to stay within the plan’s network of providers in order to receive benefits. But this is not the case with other Medigap plans.)
After the claim is processed, you’ll be able to see details in your MyMedicare.gov account . Medicare will also send you a Medicare Summary Notice. This is Medicare’s version of an explanation of benefits (EOB) , which is sent out every three months.
If you have a Medigap plan, it should also send you an EOB or something similar, explaining the claim and whether the policy paid any part of it.
What Is Medicare Assignment of Benefits?
For Medicare beneficiaries, assignment of benefits means that the person receiving care agrees to allow a nonparticipating provider to bill Medicare directly (as opposed to having the person receiving care pay the bill up front and seek reimbursement from Medicare). Assignment of benefits is authorized by the person receiving care in Box 13 of Form CMS-1500 .
If the person receiving care refuses to assign benefits, Medicare can only reimburse the person receiving care instead of paying the nonparticipating provider directly.
Things to Consider Before Choosing a Provider
If you’re enrolled in Original Medicare, you have a wide range of options in terms of the providers you can use—far more than most other Americans. In most cases, your preferred doctor and other medical providers will accept assignment with Medicare, keeping your out-of-pocket costs lower than they would otherwise be, and reducing administrative hassle.
There may be circumstances, however, when the best option is a nonparticipating provider or even a provider who has opted out of Medicare altogether. If you choose one of these options, be sure you discuss the details with the provider before proceeding with the treatment.
You’ll want to understand how much is going to be billed and whether the provider will bill Medicare on your behalf if you agree to assign benefits (note that this is not possible if the provider has opted out of Medicare).
If you have supplemental coverage, you’ll also want to check with that plan to see whether it will still pick up some of the cost and, if so, how much you should expect to pay out of your own pocket.
A medical provider who accepts Medicare assignment is considered a participating provider. These providers have agreed to accept Medicare’s fee schedule as payment in full for services they provide to Medicare beneficiaries. Most doctors, hospitals, and other medical providers do accept Medicare assignment.
Nonparticipating providers are those who have not signed an agreement with Medicare to accept Medicare’s rates as payment in full. However, they can agree to accept assignment on a case-by-case basis, as long as they haven’t opted out of Medicare altogether. If they do not accept assignment, they can bill the patient up to 15% more than the Medicare-approved rate.
Providers who opt out of Medicare cannot bill Medicare and Medicare will not pay them or reimburse beneficiaries for their services. But there is no limit on how much they can bill for their services.
A Word From Verywell
It’s in your best interest to choose a provider who accepts Medicare assignment. This will keep your costs as low as possible, streamline the billing and claims process, and ensure that your Medigap plan picks up its share of the costs.
If you feel like you need help navigating the provider options or seeking care from a provider who doesn’t accept assignment, the Medicare State Health Insurance Assistance Program (SHIP) in your state may be able to help.
A doctor who does not accept Medicare assignment has not agreed to accept Medicare’s fee schedule as payment in full for their services. These doctors are considered nonparticipating with Medicare and can bill Medicare beneficiaries up to 15% more than the Medicare-approved amount.
They also have the option to accept assignment (i.e., accept Medicare’s rate as payment in full) on a case-by-case basis.
There are certain circumstances in which a provider is required by law to accept assignment. This includes situations in which the person receiving care has both Medicare and Medicaid. And it also applies to certain medical services, including lab tests, ambulance services, and drugs that are covered under Medicare Part B (as opposed to Part D).
In 2021, 98% of American physicians had participation agreements with Medicare, leaving only about 2% who did not accept assignment (either as a nonparticipating provider, or a provider who had opted out of Medicare altogether).
Accepting assignment is something that the medical provider does, whereas assignment of benefits is something that the patient (the Medicare beneficiary) does. To accept assignment means that the medical provider has agreed to accept Medicare’s approved fee as payment in full for services they provide.
Assignment of benefits means that the person receiving care agrees to allow a medical provider to bill Medicare directly, as opposed to having the person receiving care pay the provider and then seek reimbursement from Medicare.
Centers for Medicare and Medicaid Services. Medicare monthly enrollment .
Centers for Medicare and Medicaid Services. Annual Medicare participation announcement .
Centers for Medicare and Medicaid Services. Lower costs with assignment .
Centers for Medicare and Medicaid Services. Find providers who have opted out of Medicare .
Kaiser Family Foundation. How many physicians have opted-out of the Medicare program ?
Center for Medicare Advocacy. Durable medical equipment, prosthetics, orthotics, and supplies (DMEPOS) updates .
Centers for Medicare and Medicaid Services. Check the status of a claim .
Centers for Medicare and Medicaid Services. Medicare claims processing manual. Chapter 26 - completing and processing form CMS-1500 data set .
Centers for Medicare and Medicaid Services. Ambulance fee schedule .
Centers for Medicare and Medicaid Services. Prescription drugs (outpatient) .
By Louise Norris Norris is a licensed health insurance agent, book author, and freelance writer. She graduated magna cum laude from Colorado State University.
Research Topics & Ideas: Healthcare
100+ Healthcare Research Topic Ideas To Fast-Track Your Project

Finding and choosing a strong research topic is the critical first step when it comes to crafting a high-quality dissertation, thesis or research project. If you’ve landed on this post, chances are you’re looking for a healthcare-related research topic , but aren’t sure where to start. Here, we’ll explore a variety of healthcare-related research ideas and topic thought-starters across a range of healthcare fields, including allopathic and alternative medicine, dentistry, physical therapy, optometry, pharmacology and public health.
NB – This is just the start…
The topic ideation and evaluation process has multiple steps . In this post, we’ll kickstart the process by sharing some research topic ideas within the healthcare domain. This is the starting point, but to develop a well-defined research topic, you’ll need to identify a clear and convincing research gap , along with a well-justified plan of action to fill that gap.
If you’re new to the oftentimes perplexing world of research, or if this is your first time undertaking a formal academic research project, be sure to check out our free dissertation mini-course. In it, we cover the process of writing a dissertation or thesis from start to end. Be sure to also sign up for our free webinar that explores how to find a high-quality research topic.
Overview: Healthcare Research Topics
- Allopathic medicine
- Alternative /complementary medicine
- Veterinary medicine
- Physical therapy/ rehab
- Optometry and ophthalmology
- Pharmacy and pharmacology
- Public health
- Examples of healthcare-related dissertations
Allopathic (Conventional) Medicine
- The effectiveness of telemedicine in remote elderly patient care
- The impact of stress on the immune system of cancer patients
- The effects of a plant-based diet on chronic diseases such as diabetes
- The use of AI in early cancer diagnosis and treatment
- The role of the gut microbiome in mental health conditions such as depression and anxiety
- The efficacy of mindfulness meditation in reducing chronic pain: A systematic review
- The benefits and drawbacks of electronic health records in a developing country
- The effects of environmental pollution on breast milk quality
- The use of personalized medicine in treating genetic disorders
- The impact of social determinants of health on chronic diseases in Asia
- The role of high-intensity interval training in improving cardiovascular health
- The efficacy of using probiotics for gut health in pregnant women
- The impact of poor sleep on the treatment of chronic illnesses
- The role of inflammation in the development of chronic diseases such as lupus
- The effectiveness of physiotherapy in pain control post-surgery

Topics & Ideas: Alternative Medicine
- The benefits of herbal medicine in treating young asthma patients
- The use of acupuncture in treating infertility in women over 40 years of age
- The effectiveness of homoeopathy in treating mental health disorders: A systematic review
- The role of aromatherapy in reducing stress and anxiety post-surgery
- The impact of mindfulness meditation on reducing high blood pressure
- The use of chiropractic therapy in treating back pain of pregnant women
- The efficacy of traditional Chinese medicine such as Shun-Qi-Tong-Xie (SQTX) in treating digestive disorders in China
- The impact of yoga on physical and mental health in adolescents
- The benefits of hydrotherapy in treating musculoskeletal disorders such as tendinitis
- The role of Reiki in promoting healing and relaxation post birth
- The effectiveness of naturopathy in treating skin conditions such as eczema
- The use of deep tissue massage therapy in reducing chronic pain in amputees
- The impact of tai chi on the treatment of anxiety and depression
- The benefits of reflexology in treating stress, anxiety and chronic fatigue
- The role of acupuncture in the prophylactic management of headaches and migraines

Topics & Ideas: Dentistry
- The impact of sugar consumption on the oral health of infants
- The use of digital dentistry in improving patient care: A systematic review
- The efficacy of orthodontic treatments in correcting bite problems in adults
- The role of dental hygiene in preventing gum disease in patients with dental bridges
- The impact of smoking on oral health and tobacco cessation support from UK dentists
- The benefits of dental implants in restoring missing teeth in adolescents
- The use of lasers in dental procedures such as root canals
- The efficacy of root canal treatment using high-frequency electric pulses in saving infected teeth
- The role of fluoride in promoting remineralization and slowing down demineralization
- The impact of stress-induced reflux on oral health
- The benefits of dental crowns in restoring damaged teeth in elderly patients
- The use of sedation dentistry in managing dental anxiety in children
- The efficacy of teeth whitening treatments in improving dental aesthetics in patients with braces
- The role of orthodontic appliances in improving well-being
- The impact of periodontal disease on overall health and chronic illnesses

Tops & Ideas: Veterinary Medicine
- The impact of nutrition on broiler chicken production
- The role of vaccines in disease prevention in horses
- The importance of parasite control in animal health in piggeries
- The impact of animal behaviour on welfare in the dairy industry
- The effects of environmental pollution on the health of cattle
- The role of veterinary technology such as MRI in animal care
- The importance of pain management in post-surgery health outcomes
- The impact of genetics on animal health and disease in layer chickens
- The effectiveness of alternative therapies in veterinary medicine: A systematic review
- The role of veterinary medicine in public health: A case study of the COVID-19 pandemic
- The impact of climate change on animal health and infectious diseases in animals
- The importance of animal welfare in veterinary medicine and sustainable agriculture
- The effects of the human-animal bond on canine health
- The role of veterinary medicine in conservation efforts: A case study of Rhinoceros poaching in Africa
- The impact of veterinary research of new vaccines on animal health
Topics & Ideas: Physical Therapy/Rehab
- The efficacy of aquatic therapy in improving joint mobility and strength in polio patients
- The impact of telerehabilitation on patient outcomes in Germany
- The effect of kinesiotaping on reducing knee pain and improving function in individuals with chronic pain
- A comparison of manual therapy and yoga exercise therapy in the management of low back pain
- The use of wearable technology in physical rehabilitation and the impact on patient adherence to a rehabilitation plan
- The impact of mindfulness-based interventions in physical therapy in adolescents
- The effects of resistance training on individuals with Parkinson’s disease
- The role of hydrotherapy in the management of fibromyalgia
- The impact of cognitive-behavioural therapy in physical rehabilitation for individuals with chronic pain
- The use of virtual reality in physical rehabilitation of sports injuries
- The effects of electrical stimulation on muscle function and strength in athletes
- The role of physical therapy in the management of stroke recovery: A systematic review
- The impact of pilates on mental health in individuals with depression
- The use of thermal modalities in physical therapy and its effectiveness in reducing pain and inflammation
- The effect of strength training on balance and gait in elderly patients
Topics & Ideas: Optometry & Opthalmology
- The impact of screen time on the vision and ocular health of children under the age of 5
- The effects of blue light exposure from digital devices on ocular health
- The role of dietary interventions, such as the intake of whole grains, in the management of age-related macular degeneration
- The use of telemedicine in optometry and ophthalmology in the UK
- The impact of myopia control interventions on African American children’s vision
- The use of contact lenses in the management of dry eye syndrome: different treatment options
- The effects of visual rehabilitation in individuals with traumatic brain injury
- The role of low vision rehabilitation in individuals with age-related vision loss: challenges and solutions
- The impact of environmental air pollution on ocular health
- The effectiveness of orthokeratology in myopia control compared to contact lenses
- The role of dietary supplements, such as omega-3 fatty acids, in ocular health
- The effects of ultraviolet radiation exposure from tanning beds on ocular health
- The impact of computer vision syndrome on long-term visual function
- The use of novel diagnostic tools in optometry and ophthalmology in developing countries
- The effects of virtual reality on visual perception and ocular health: an examination of dry eye syndrome and neurologic symptoms
Topics & Ideas: Pharmacy & Pharmacology
- The impact of medication adherence on patient outcomes in cystic fibrosis
- The use of personalized medicine in the management of chronic diseases such as Alzheimer’s disease
- The effects of pharmacogenomics on drug response and toxicity in cancer patients
- The role of pharmacists in the management of chronic pain in primary care
- The impact of drug-drug interactions on patient mental health outcomes
- The use of telepharmacy in healthcare: Present status and future potential
- The effects of herbal and dietary supplements on drug efficacy and toxicity
- The role of pharmacists in the management of type 1 diabetes
- The impact of medication errors on patient outcomes and satisfaction
- The use of technology in medication management in the USA
- The effects of smoking on drug metabolism and pharmacokinetics: A case study of clozapine
- Leveraging the role of pharmacists in preventing and managing opioid use disorder
- The impact of the opioid epidemic on public health in a developing country
- The use of biosimilars in the management of the skin condition psoriasis
- The effects of the Affordable Care Act on medication utilization and patient outcomes in African Americans
Topics & Ideas: Public Health
- The impact of the built environment and urbanisation on physical activity and obesity
- The effects of food insecurity on health outcomes in Zimbabwe
- The role of community-based participatory research in addressing health disparities
- The impact of social determinants of health, such as racism, on population health
- The effects of heat waves on public health
- The role of telehealth in addressing healthcare access and equity in South America
- The impact of gun violence on public health in South Africa
- The effects of chlorofluorocarbons air pollution on respiratory health
- The role of public health interventions in reducing health disparities in the USA
- The impact of the United States Affordable Care Act on access to healthcare and health outcomes
- The effects of water insecurity on health outcomes in the Middle East
- The role of community health workers in addressing healthcare access and equity in low-income countries
- The impact of mass incarceration on public health and behavioural health of a community
- The effects of floods on public health and healthcare systems
- The role of social media in public health communication and behaviour change in adolescents
Examples: Healthcare Dissertation & Theses
While the ideas we’ve presented above are a decent starting point for finding a healthcare-related research topic, they are fairly generic and non-specific. So, it helps to look at actual dissertations and theses to see how this all comes together.
Below, we’ve included a selection of research projects from various healthcare-related degree programs to help refine your thinking. These are actual dissertations and theses, written as part of Master’s and PhD-level programs, so they can provide some useful insight as to what a research topic looks like in practice.
- Improving Follow-Up Care for Homeless Populations in North County San Diego (Sanchez, 2021)
- On the Incentives of Medicare’s Hospital Reimbursement and an Examination of Exchangeability (Elzinga, 2016)
- Managing the healthcare crisis: the career narratives of nurses (Krueger, 2021)
- Methods for preventing central line-associated bloodstream infection in pediatric haematology-oncology patients: A systematic literature review (Balkan, 2020)
- Farms in Healthcare: Enhancing Knowledge, Sharing, and Collaboration (Garramone, 2019)
- When machine learning meets healthcare: towards knowledge incorporation in multimodal healthcare analytics (Yuan, 2020)
- Integrated behavioural healthcare: The future of rural mental health (Fox, 2019)
- Healthcare service use patterns among autistic adults: A systematic review with narrative synthesis (Gilmore, 2021)
- Mindfulness-Based Interventions: Combatting Burnout and Compassionate Fatigue among Mental Health Caregivers (Lundquist, 2022)
- Transgender and gender-diverse people’s perceptions of gender-inclusive healthcare access and associated hope for the future (Wille, 2021)
- Efficient Neural Network Synthesis and Its Application in Smart Healthcare (Hassantabar, 2022)
- The Experience of Female Veterans and Health-Seeking Behaviors (Switzer, 2022)
- Machine learning applications towards risk prediction and cost forecasting in healthcare (Singh, 2022)
- Does Variation in the Nursing Home Inspection Process Explain Disparity in Regulatory Outcomes? (Fox, 2020)
Looking at these titles, you can probably pick up that the research topics here are quite specific and narrowly-focused , compared to the generic ones presented earlier. This is an important thing to keep in mind as you develop your own research topic. That is to say, to create a top-notch research topic, you must be precise and target a specific context with specific variables of interest . In other words, you need to identify a clear, well-justified research gap.
Need more help?
If you’re still feeling a bit unsure about how to find a research topic for your healthcare dissertation or thesis, check out Topic Kickstarter service below.

You Might Also Like:

15 Comments

I need topics that will match the Msc program am running in healthcare research please

Hello Mabel,
I can help you with a good topic, kindly provide your email let’s have a good discussion on this.

Can you provide some research topics and ideas on Immunology?

Thank you to create new knowledge on research problem verse research topic
Help on problem statement on teen pregnancy

This post might be useful: https://gradcoach.com/research-problem-statement/

can you provide me with a research topic on healthcare related topics to a qqi level 5 student

Please can someone help me with research topics in public health ?

Hello I have requirement of Health related latest research issue/topics for my social media speeches. If possible pls share health issues , diagnosis, treatment.

I would like a topic thought around first-line support for Gender-Based Violence for survivors or one related to prevention of Gender-Based Violence

Please can I be helped with a master’s research topic in either chemical pathology or hematology or immunology? thanks

Can u please provide me with a research topic on occupational health and safety at the health sector

Good day kindly help provide me with Ph.D. Public health topics on Reproductive and Maternal Health, interventional studies on Health Education

may you assist me with a good easy healthcare administration study topic

May you assist me in finding a research topic on nutrition,physical activity and obesity. On the impact on children
Submit a Comment Cancel reply
Your email address will not be published. Required fields are marked *
Save my name, email, and website in this browser for the next time I comment.
- Print Friendly
- Account Settings
FEATURED INSIGHTS
- Behavioral health
- Site-of-care shifts
- Specialty care
- State of the healthcare industry
- The workforce crisis
- Value-based care
- View all featured insights
RESOURCES BY SECTOR
- Digital health
- Health plans
- Hospitals and health systems
- Medical device
- Physicians and medical groups
- Purchased and professional services
- View all sectors
NEWS & INSIGHTS
- Daily Briefing
- Radio Advisory
- Advisory Board tools
PRODUCTS & SERVICES
- Research Membership
- Expert Support
- Advisory Board Fellowship
- On-Demand Courses
- Sponsorship
FEATURED CONTENT
Truly personalized care is possible. here's how to make it a reality..
Learn to navigate 4 key obstacles to improve patient access to innovative care.

- AskAdvisory
Our direct-to-expert service is here to help you navigate your membership, our research, and your most pressing challenges in healthcare. No question is too big or too small.
The 6 challenges facing health care in 2023—and how to handle them
With input from stakeholders across the industry, Modern Healthcare outlines six challenges health care is likely to face in 2023—and what leaders can do about them.
1. Financial difficulties
In 2023, health systems will likely continue to face financial difficulties due to ongoing staffing problems, reduced patient volumes, and rising inflation.
According to Tina Wheeler, U.S. health care leader at Deloitte , hospitals can expect wage growth to continue to increase even as they try to contain labor costs. They can also expect expenses, including for supplies and pharmaceuticals, to remain elevated.
Health systems are also no longer able to rely on federal Covid-19 relief funding to offset some of these rising costs. Cuts to Medicare reimbursement rates could also negatively impact revenue.
"You're going to have all these forces that are counterproductive that you're going to have to navigate," Wheeler said.
In addition, Erik Swanson, SVP of data and analytics at Kaufman Hall , said the continued shift to outpatient care will likely affect hospitals' profit margins.
"The reality is … those sites of care in many cases tend to be lower-cost ways of delivering care, so ultimately it could be beneficial to health systems as a whole, but only for those systems that are able to offer those services and have that footprint," he said.
2. Health system mergers
Although hospital transactions have slowed in the last few years, market watchers say mergers are expected to rebound as health systems aim to spread their growing expenses over larger organizations and increase their bargaining leverage with insurers.
"There is going to be some organizational soul-searching for some health systems that might force them to affiliate, even though they prefer not to," said Patrick Cross, a partner at Faegre Drinker Biddle & Reath . "Health systems are soliciting partners, not because they are on the verge of bankruptcy, but because they are looking at their crystal ball and not seeing an easy road ahead."
Financial challenges may also lead more physician practices to join health systems, private-equity groups, larger practices, or insurance companies.
"Many independent physicians are really struggling with their ability to maintain their independence," said Joshua Kaye, chair of U.S. health care practice at DLA Piper . "There will be a fair amount of deal activity. The question will be more about the size and specialty of the practices that will be part of the next consolidation wave."
3. Recruiting and retaining staff
According to data from Fitch Ratings , health care job openings reached an all-time high of 9.2% in September 2022—more than double the average rate of 4.2% between 2010 and 2019. With this trend likely to continue, organizations will need to find effective ways to recruit and retain workers.
Currently, some organizations are upgrading their processes and technology to hire people more quickly. They are also creating service-level agreements between recruiting and hiring teams to ensure interviews are scheduled within 48 hours or decisions are made within 24 hours.
Eric Burch, executive principal of operations and workforce services at Vizient , also predicted that there will be a continued need for contract labors, so health systems will need to consider travel nurses in their staffing plans.
"It's really important to approach contract labor vendors as a strategic partner," Burch said. "So when you need the staff, it's a partnership and they're able to help you get to your goals, versus suddenly reaching out to them and they don’t know your needs when you're in crisis."
When it comes to retention, Tochi Iroku-Malize, president of the American Academy of Family Physicians (AAFP), said health systems are adequately compensated for their work and have enough staff to alleviate potential burnout.
AAFP also supports legislation to streamline prior authorization in the Medicare Advantage program and avoid additional cuts to Medicare payments, which will help physicians provide care to patients with less stress.
4. Payer-provider contract disputes
A potential recession, along with the ensuing job cuts that typically follow, would limit insurers' commercial business, which is their most profitable product line. Instead, many people who lose their jobs will likely sign up for Medicaid plans, which is much less profitable.
Because of increased labor, supply, and infrastructure costs, Brad Ellis, senior director at Fitch Ratings, said providers could pressure insurers into increasing the amount they pay for services. This will lead insurers to passing these increased costs onto members' premiums.
Currently, Ellis said insurers are keeping an eye on how legislators finalize rules to implement the No Surprise Act's independent resolution process. Regulators will also begin issuing fines for payers who are not in compliance with the law's price transparency requirement.
5. Investment in digital health
Much like 2022, investment in digital health is likely to remain strong but subdued in 2023.
"You'll continue to see layoffs, and startup funding is going to be hard to come by," said Russell Glass, CEO of Headspace Health .
However, investors and health care leaders say they expect a strong market for digital health technology, such as tools for revenue cycle management and hospital-at-home programs.
According to Julian Pham, founding and managing partner at Third Culture Capital , he expects corporations such as CVS Health to continue to invest in health tech companies and for there to be more digital health mergers and acquisitions overall.
In addition, he predicted that investors, pharmaceutical companies, and insurers will show more interest in digital therapeutics, which are software applications prescribed by clinicians.
"As a physician, I’ve always dreamed of a future where I could prescribe an app," Pham said. "Is it the right time? Time will tell. A lot needs to happen in digital therapeutics and it's going to be hard."
6. Health equity efforts
This year, CMS will continue rolling out new health equity initiatives and quality measurements for providers and insurers who serve marketplace, Medicare, and Medicaid beneficiaries. Some new quality measures include maternal health, opioid related adverse events, and social need/risk factor screenings.
CMS, the Joint Commission , and the National Committee for Quality Assurance are also partnering together to establish standards for health equity and data collection.
In addition, HHS is slated to restore a rule under the Affordable Care Act that prohibits discrimination based on a person's gender identity or sexual orientation. According to experts, this rule may conflict with recently passed state laws that ban gender-affirming care for minors.
"It's something that's going to bear out in the courts and will likely lack clarity. We'll see differences in what different courts decide," said Lindsey Dawson, associate director of HIV policy and director of LGBTQ health policy at the Kaiser Family Foundation . "The Supreme Court acknowledged that there was this tension. So it's an important place to watch and understand better moving forward." (Devereaux et al., Modern Healthcare , 1/2)
Is this content helpful?
Posted on January 04, 2023
Updated on March 17, 2023
Around the nation: FDA updates 'morning after' pill's label
What caused this nfl player to collapse during a game here's what experts say., what a congressional investigation reveals about fda's approval of aduhelm, a 19-year-old man developed a 'strange rash' before noticing blood in his urine. what was wrong, invasive strep a infections are rising. here's what you need to know..
We help leaders and future leaders in the healthcare industry work smarter and faster by providing provocative insights, actionable strategies, and practical tools to support execution.
- All Resources
- Our History
- Legal Disclaimer
- Privacy Policy
- Terms of Use
Don't miss out on the latest Advisory Board insights
Create your free account to access 2 resources each month, including the latest research and webinars.
Want access without creating an account?
You have 2 free members-only resources remaining this month remaining this month.
1 free members-only resources remaining this month
You've reached your limit of free monthly insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
- Skip to main content
- Keyboard shortcuts for audio player
Patients die every day waiting for organ transplants. The problem goes beyond donations

Scott Simon
NPR's Scott Simon speaks with Jennifer Erickson, senior fellow with the Federation of American Scientists, about the organ transplant system and how eligible donated organs wind up in the trash.
SCOTT SIMON, HOST:
A major hospital brought its kidney and liver transplant program to a halt this week. Memorial Hermann-Texas Medical Center said its waiting lists had been manipulated, so some patients were effectively pushed out of line. The federal government says it's investigating, but even without suspected misconduct, 17 patients die each day while on similar waiting lists. And although it can mean life or death for patients, a senior fellow at the Federation of American Scientists says that too many eligible organs just wind up in the trash. Jennifer Erickson also worked in the Obama administration and joins us in our studios. Thanks so much for being with us.
JENNIFER ERICKSON: Thanks for having me.
SIMON: These are organs that could save lives. How do they wind up in the trash?
ERICKSON: Oh, gosh. Well, they don't get there in time. There was a surgeon who testified before the Senate about receiving a kidney in a box with tire marks on it. Organs can be recovered by people with no clinical experience. So someone might recover an organ from a generous organ donor but make a mistake in how they cut it out. I mean, Scott, you could be recovering organs tomorrow. You're a great radio interviewer, but I'm sure you would agree that we should actually have clinicians doing that work. And that isn't actually what the federal government requires.
SIMON: Congress created the organ donation system in the 1980s. How does that affect what we're seeing with organs being donated and then winding up in the trash?
ERICKSON: Well, the central flaw of how the system was set up is that it's run by a network of monopoly contractors. Every single monopoly that got a contract from the federal government in the 1980s is still there 40 years later, and has never, not once, faced competition or accountability - not for Medicare fraud, not for deadly patient safety lapses, not for their organs that they've recovered ending up in the trash. It's just year after year, the taxpayers send them a check, and they don't have to be accountable for the job they actually do.
SIMON: You say monopoly, but as you note, it's government funded, so technically, it's a centralized system.
ERICKSON: So there's 55 local monopolies. Those are called organ procurement organizations. They are the folks that are supposed to turn up at a hospital every potential time to honor a potential organ donation wish. But too often, they don't show up. And then there's a national contractor, one to look out for all the others, and that is the United Network for Organ Sharing, or UNOS. And they have just been an abject failure for the last 40 years.
SIMON: Don't all these companies have - forgive me - a financial incentive to talk to people and to deliver organs?
ERICKSON: They actually don't because organ procurement organizations are one of the last remaining parts of U.S. health care that are funded on a cost-reimbursement basis. They are not funded based on how many organs they recover or on how many organs are successfully transplanted. They're just refunded for whatever they spent. So if they buy private planes, if they have multimillion-dollar CEO salaries, it all just goes on to the payer, which is usually the taxpayer, and it's completely divorced from how they actually serve patients.
SIMON: What needs to be done, in your estimation?
ERICKSON: The Centers for Medicare & Medicaid Services has said that 74% of the nation's organ recovery agencies are failing performance standards, yet none of them has ever lost a contract. The government actually has to stand up for patients. It has to say, if you're one of the 20-odd percent that's doing the job, keep doing it. And if not, replace them immediately 'cause these are lives at stake.
SIMON: I was on a flight this week that was delayed six hours. Probably hundreds of thousands of other people were. For all I know, there was an organ being transplanted, and maybe by the time it actually arrived, it was unusable for one reason or another. I can imagine a contractor saying, look, that was the fault of American Airlines, not us.
ERICKSON: OK. Well, I'll give you a statistic back then. The national monopoly, UNOS, is 15 times more likely to lose or damage an organ in transit than an airline is a suitcase. For organs, it's absolutely objectively worse.
SIMON: What do you hope an organ donation system can ultimately look like, you know, recognizing there will be transportation delays and surgical mistakes and all human factors.
ERICKSON: I hope it's safe. I hope it's equitable. I hope that organ donation wishes are honored, and I think it just goes back to that reality that monopolies don't work. And I'll give you a glimmer of hope here. Last July, Congress voted unanimously to break up the national monopoly contract held by UNOS. So now what we need is the agencies within the Department of Health and Human Services to actually finish the job. They have to remember that, like you said, every day, we have - it's actually more than 17 Americans die waiting. If you take those who've already been removed from the waiting list because they're too sick to transplant, 30 Americans die every day. And it's not because the organs aren't available. It's because the system they've probably never heard of isn't doing its job.
SIMON: Jennifer Erickson, senior fellow at the Federation of American Scientists. Thank you so much for being with us.
ERICKSON: Thank you.
(SOUNDBITE OF MUSIC)
Copyright © 2024 NPR. All rights reserved. Visit our website terms of use and permissions pages at www.npr.org for further information.
NPR transcripts are created on a rush deadline by an NPR contractor. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of NPR’s programming is the audio record.
An official website of the United States government
Here’s how you know
Official websites use .gov A .gov website belongs to an official government organization in the United States.
Secure .gov websites use HTTPS A lock ( Lock Locked padlock icon ) or https:// means you’ve safely connected to the .gov website. Share sensitive information only on official, secure websites.
- Entire Site
- Research & Funding
- Health Information
- About NIDDK
- Diabetes Overview
Healthy Living with Diabetes
- Español
On this page:
How can I plan what to eat or drink when I have diabetes?
How can physical activity help manage my diabetes, what can i do to reach or maintain a healthy weight, should i quit smoking, how can i take care of my mental health, clinical trials for healthy living with diabetes.
Healthy living is a way to manage diabetes . To have a healthy lifestyle, take steps now to plan healthy meals and snacks, do physical activities, get enough sleep, and quit smoking or using tobacco products.
Healthy living may help keep your body’s blood pressure , cholesterol , and blood glucose level, also called blood sugar level, in the range your primary health care professional recommends. Your primary health care professional may be a doctor, a physician assistant, or a nurse practitioner. Healthy living may also help prevent or delay health problems from diabetes that can affect your heart, kidneys, eyes, brain, and other parts of your body.
Making lifestyle changes can be hard, but starting with small changes and building from there may benefit your health. You may want to get help from family, loved ones, friends, and other trusted people in your community. You can also get information from your health care professionals.
What you choose to eat, how much you eat, and when you eat are parts of a meal plan. Having healthy foods and drinks can help keep your blood glucose, blood pressure, and cholesterol levels in the ranges your health care professional recommends. If you have overweight or obesity, a healthy meal plan—along with regular physical activity, getting enough sleep, and other healthy behaviors—may help you reach and maintain a healthy weight. In some cases, health care professionals may also recommend diabetes medicines that may help you lose weight, or weight-loss surgery, also called metabolic and bariatric surgery.
Choose healthy foods and drinks
There is no right or wrong way to choose healthy foods and drinks that may help manage your diabetes. Healthy meal plans for people who have diabetes may include
- dairy or plant-based dairy products
- nonstarchy vegetables
- protein foods
- whole grains
Try to choose foods that include nutrients such as vitamins, calcium , fiber , and healthy fats . Also try to choose drinks with little or no added sugar , such as tap or bottled water, low-fat or non-fat milk, and unsweetened tea, coffee, or sparkling water.
Try to plan meals and snacks that have fewer
- foods high in saturated fat
- foods high in sodium, a mineral found in salt
- sugary foods , such as cookies and cakes, and sweet drinks, such as soda, juice, flavored coffee, and sports drinks
Your body turns carbohydrates , or carbs, from food into glucose, which can raise your blood glucose level. Some fruits, beans, and starchy vegetables—such as potatoes and corn—have more carbs than other foods. Keep carbs in mind when planning your meals.
You should also limit how much alcohol you drink. If you take insulin or certain diabetes medicines , drinking alcohol can make your blood glucose level drop too low, which is called hypoglycemia . If you do drink alcohol, be sure to eat food when you drink and remember to check your blood glucose level after drinking. Talk with your health care team about your alcohol-drinking habits.

Find the best times to eat or drink
Talk with your health care professional or health care team about when you should eat or drink. The best time to have meals and snacks may depend on
- what medicines you take for diabetes
- what your level of physical activity or your work schedule is
- whether you have other health conditions or diseases
Ask your health care team if you should eat before, during, or after physical activity. Some diabetes medicines, such as sulfonylureas or insulin, may make your blood glucose level drop too low during exercise or if you skip or delay a meal.
Plan how much to eat or drink
You may worry that having diabetes means giving up foods and drinks you enjoy. The good news is you can still have your favorite foods and drinks, but you might need to have them in smaller portions or enjoy them less often.
For people who have diabetes, carb counting and the plate method are two common ways to plan how much to eat or drink. Talk with your health care professional or health care team to find a method that works for you.
Carb counting
Carbohydrate counting , or carb counting, means planning and keeping track of the amount of carbs you eat and drink in each meal or snack. Not all people with diabetes need to count carbs. However, if you take insulin, counting carbs can help you know how much insulin to take.
Plate method
The plate method helps you control portion sizes without counting and measuring. This method divides a 9-inch plate into the following three sections to help you choose the types and amounts of foods to eat for each meal.
- Nonstarchy vegetables—such as leafy greens, peppers, carrots, or green beans—should make up half of your plate.
- Carb foods that are high in fiber—such as brown rice, whole grains, beans, or fruits—should make up one-quarter of your plate.
- Protein foods—such as lean meats, fish, dairy, or tofu or other soy products—should make up one quarter of your plate.
If you are not taking insulin, you may not need to count carbs when using the plate method.

Work with your health care team to create a meal plan that works for you. You may want to have a diabetes educator or a registered dietitian on your team. A registered dietitian can provide medical nutrition therapy , which includes counseling to help you create and follow a meal plan. Your health care team may be able to recommend other resources, such as a healthy lifestyle coach, to help you with making changes. Ask your health care team or your insurance company if your benefits include medical nutrition therapy or other diabetes care resources.
Talk with your health care professional before taking dietary supplements
There is no clear proof that specific foods, herbs, spices, or dietary supplements —such as vitamins or minerals—can help manage diabetes. Your health care professional may ask you to take vitamins or minerals if you can’t get enough from foods. Talk with your health care professional before you take any supplements, because some may cause side effects or affect how well your diabetes medicines work.
Research shows that regular physical activity helps people manage their diabetes and stay healthy. Benefits of physical activity may include
- lower blood glucose, blood pressure, and cholesterol levels
- better heart health
- healthier weight
- better mood and sleep
- better balance and memory
Talk with your health care professional before starting a new physical activity or changing how much physical activity you do. They may suggest types of activities based on your ability, schedule, meal plan, interests, and diabetes medicines. Your health care professional may also tell you the best times of day to be active or what to do if your blood glucose level goes out of the range recommended for you.

Do different types of physical activity
People with diabetes can be active, even if they take insulin or use technology such as insulin pumps .
Try to do different kinds of activities . While being more active may have more health benefits, any physical activity is better than none. Start slowly with activities you enjoy. You may be able to change your level of effort and try other activities over time. Having a friend or family member join you may help you stick to your routine.
The physical activities you do may need to be different if you are age 65 or older , are pregnant , or have a disability or health condition . Physical activities may also need to be different for children and teens . Ask your health care professional or health care team about activities that are safe for you.
Aerobic activities
Aerobic activities make you breathe harder and make your heart beat faster. You can try walking, dancing, wheelchair rolling, or swimming. Most adults should try to get at least 150 minutes of moderate-intensity physical activity each week. Aim to do 30 minutes a day on most days of the week. You don’t have to do all 30 minutes at one time. You can break up physical activity into small amounts during your day and still get the benefit. 1
Strength training or resistance training
Strength training or resistance training may make your muscles and bones stronger. You can try lifting weights or doing other exercises such as wall pushups or arm raises. Try to do this kind of training two times a week. 1
Balance and stretching activities
Balance and stretching activities may help you move better and have stronger muscles and bones. You may want to try standing on one leg or stretching your legs when sitting on the floor. Try to do these kinds of activities two or three times a week. 1
Some activities that need balance may be unsafe for people with nerve damage or vision problems caused by diabetes. Ask your health care professional or health care team about activities that are safe for you.

Stay safe during physical activity
Staying safe during physical activity is important. Here are some tips to keep in mind.
Drink liquids
Drinking liquids helps prevent dehydration , or the loss of too much water in your body. Drinking water is a way to stay hydrated. Sports drinks often have a lot of sugar and calories , and you don’t need them for most moderate physical activities.
Avoid low blood glucose
Check your blood glucose level before, during, and right after physical activity. Physical activity often lowers the level of glucose in your blood. Low blood glucose levels may last for hours or days after physical activity. You are most likely to have low blood glucose if you take insulin or some other diabetes medicines, such as sulfonylureas.
Ask your health care professional if you should take less insulin or eat carbs before, during, or after physical activity. Low blood glucose can be a serious medical emergency that must be treated right away. Take steps to protect yourself. You can learn how to treat low blood glucose , let other people know what to do if you need help, and use a medical alert bracelet.
Avoid high blood glucose and ketoacidosis
Taking less insulin before physical activity may help prevent low blood glucose, but it may also make you more likely to have high blood glucose. If your body does not have enough insulin, it can’t use glucose as a source of energy and will use fat instead. When your body uses fat for energy, your body makes chemicals called ketones .
High levels of ketones in your blood can lead to a condition called diabetic ketoacidosis (DKA) . DKA is a medical emergency that should be treated right away. DKA is most common in people with type 1 diabetes . Occasionally, DKA may affect people with type 2 diabetes who have lost their ability to produce insulin. Ask your health care professional how much insulin you should take before physical activity, whether you need to test your urine for ketones, and what level of ketones is dangerous for you.
Take care of your feet
People with diabetes may have problems with their feet because high blood glucose levels can damage blood vessels and nerves. To help prevent foot problems, wear comfortable and supportive shoes and take care of your feet before, during, and after physical activity.

If you have diabetes, managing your weight may bring you several health benefits. Ask your health care professional or health care team if you are at a healthy weight or if you should try to lose weight.
If you are an adult with overweight or obesity, work with your health care team to create a weight-loss plan. Losing 5% to 7% of your current weight may help you prevent or improve some health problems and manage your blood glucose, cholesterol, and blood pressure levels. 2 If you are worried about your child’s weight and they have diabetes, talk with their health care professional before your child starts a new weight-loss plan.
You may be able to reach and maintain a healthy weight by
- following a healthy meal plan
- consuming fewer calories
- being physically active
- getting 7 to 8 hours of sleep each night 3
If you have type 2 diabetes, your health care professional may recommend diabetes medicines that may help you lose weight.
Online tools such as the Body Weight Planner may help you create eating and physical activity plans. You may want to talk with your health care professional about other options for managing your weight, including joining a weight-loss program that can provide helpful information, support, and behavioral or lifestyle counseling. These options may have a cost, so make sure to check the details of the programs.
Your health care professional may recommend weight-loss surgery if you aren’t able to reach a healthy weight with meal planning, physical activity, and taking diabetes medicines that help with weight loss.
If you are pregnant , trying to lose weight may not be healthy. However, you should ask your health care professional whether it makes sense to monitor or limit your weight gain during pregnancy.
Both diabetes and smoking —including using tobacco products and e-cigarettes—cause your blood vessels to narrow. Both diabetes and smoking increase your risk of having a heart attack or stroke , nerve damage , kidney disease , eye disease , or amputation . Secondhand smoke can also affect the health of your family or others who live with you.
If you smoke or use other tobacco products, stop. Ask for help . You don’t have to do it alone.
Feeling stressed, sad, or angry can be common for people with diabetes. Managing diabetes or learning to cope with new information about your health can be hard. People with chronic illnesses such as diabetes may develop anxiety or other mental health conditions .
Learn healthy ways to lower your stress , and ask for help from your health care team or a mental health professional. While it may be uncomfortable to talk about your feelings, finding a health care professional whom you trust and want to talk with may help you
- lower your feelings of stress, depression, or anxiety
- manage problems sleeping or remembering things
- see how diabetes affects your family, school, work, or financial situation
Ask your health care team for mental health resources for people with diabetes.
Sleeping too much or too little may raise your blood glucose levels. Your sleep habits may also affect your mental health and vice versa. People with diabetes and overweight or obesity can also have other health conditions that affect sleep, such as sleep apnea , which can raise your blood pressure and risk of heart disease.

NIDDK conducts and supports clinical trials in many diseases and conditions, including diabetes. The trials look to find new ways to prevent, detect, or treat disease and improve quality of life.
What are clinical trials for healthy living with diabetes?
Clinical trials—and other types of clinical studies —are part of medical research and involve people like you. When you volunteer to take part in a clinical study, you help health care professionals and researchers learn more about disease and improve health care for people in the future.
Researchers are studying many aspects of healthy living for people with diabetes, such as
- how changing when you eat may affect body weight and metabolism
- how less access to healthy foods may affect diabetes management, other health problems, and risk of dying
- whether low-carbohydrate meal plans can help lower blood glucose levels
- which diabetes medicines are more likely to help people lose weight
Find out if clinical trials are right for you .
Watch a video of NIDDK Director Dr. Griffin P. Rodgers explaining the importance of participating in clinical trials.
What clinical trials for healthy living with diabetes are looking for participants?
You can view a filtered list of clinical studies on healthy living with diabetes that are federally funded, open, and recruiting at www.ClinicalTrials.gov . You can expand or narrow the list to include clinical studies from industry, universities, and individuals; however, the National Institutes of Health does not review these studies and cannot ensure they are safe for you. Always talk with your primary health care professional before you participate in a clinical study.
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. NIDDK translates and disseminates research findings to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by NIDDK is carefully reviewed by NIDDK scientists and other experts.
NIDDK would like to thank: Elizabeth M. Venditti, Ph.D., University of Pittsburgh School of Medicine.
Arizona's 1864 abortion ban was mostly a result of power struggles, historians say

Attempts to gain power mostly fueled Arizona’s near-total abortion ban in 1864, as male physicians sought to dominate health care over midwives and anti-abortion advocates felt threatened by immigrants, historians said.
The Civil War-era law — which the state Supreme Court this week ruled was enforceable — was enacted at a time when women did not have the right to vote and before Arizona, then a territory, became a state.
Back then, midwives predominantly performed abortions, using herbs or metal instruments, which caused resentment among male physicians, said Karissa Haugeberg, who teaches history at Tulane University in Louisiana.
“Physicians marked midwives as competitors,” Haugeberg said. So they began campaigning to be the authorities on reproductive rights and health care.
In 1847, a small group of physicians formed the American Medical Association, largely to quash competition from midwives and other nonlicensed providers while boosting their standing as a trustworthy and well-regulated guild, said Christopher Griffin, the director of empirical and policy research at the University of Arizona.
Haugeberg said, “A lot of this was this, like, behind-the-scenes battle of physicians trying to corner the market on obstetrical care and put the decision-making power of abortion in their hands.”
At the same time, rising birthrates among an influx of Catholic immigrants, coupled with dramatically falling birthrates among American-born women, sparked “replacement theory” concerns.
“There was a huge fear, a very xenophobic fear,” Haugeberg said. “Part of it was truly to control the fertility of American-born women.”
Some abortion restrictions were already in place at the time Arizona's passed, said Jill Wieber Lens, a University of Arkansas law professor who studies reproductive rights.
Before the state's near-total ban, abortions were illegal there only after women started to feel fetal movement, which Lens said could begin between 16 and 21 weeks' gestation.
But the AMA and other powerful anti-abortion advocates began a crusade against abortion in the late 1850s. And within a decade, a national movement to restrict it gained momentum.
“You can start to see the beginnings of what we now call the right-to-life movement,” Griffin said.
The Arizona law in 1864 made abortion before the detection of fetal movement a felony, punishable by two to five years in prison for anyone who performed an abortion or helped a woman obtain one, except to save the woman’s life.
A wave of similar bans swept the country. By the end of the 19th century, Haugeberg said, every state and territory had criminalized abortion.
Mary Ziegler, a legal historian at the University of California, Davis School of Law, said, “These laws all passed at the behest of the AMA, which wanted more power and discretion.”
“And that’s what these laws gave them," she said.
The AMA said its stance on abortion has “evolved substantially since its early days in the 1800s.” In the last 50 years, it said, it has been an “advocate in defending the practice of medicine,” and it said it believes the early termination of a pregnancy is a medical matter between a patient and a physician.
And while the ban gave physicians more power in the 1860s, today’s national abortion restrictions leave doctors uncertain about when they can render care without being prosecuted, Ziegler said.
The Arizona Supreme Court said Tuesday it would put its decision on hold for 14 days so a lower court can consider “additional constitutional challenges.” Assuming the 1864 policy once again becomes state law, Arizona would be the latest state to effectively ban abortion care.
“It’s really stunning to uphold a law that at its very heart is so gendered,” Haugeberg said. “It seems to ignore all of the movement we’ve made for equality.”
In the 1860s, birth control and pregnancy tests did not exist, and what would today be considered an early-term abortion was a somewhat common practice. Doctors had a limited understanding of reproductive health, and technology lagged, historical experts said.
It was not for another 60 years that researchers would begin testing for pregnancy by injecting women’s urine into young rats to identify hormone reactions.
“That was the best science we had,” Lens said. “People today can’t even imagine it.”
Melissa Chan is a reporter for NBC News Digital with a focus on veterans’ issues, mental health in the military and gun violence.
The assignment-dial-a-ride-problem
- Published: 21 October 2023
- Volume 26 , pages 770–784, ( 2023 )
Cite this article
- Chane-Haï Timothée 1 ,
- Vercraene Samuel 1 &
- Monteiro Thibaud ORCID: orcid.org/0000-0002-6301-7403 1
213 Accesses
Explore all metrics
In this paper, we present the first Assignment-Dial-A-Ride problem motivated by a real-life problem faced by medico-social institutions in France. Every day, disabled people use ride-sharing services to go to an appropriate institution where they receive personal care. These institutions have to manage their staff to meet the demands of the people they receive. They have to solve three interconnected problems: the routing for the ride-sharing services; the assignment of disabled people to institutions; and the staff size in the institutions. We formulate a general Assignment-Dial-A-Ride problem to solve all three at the same time. We first present a matheuristic that iteratively generates routes using a large neighborhood search in which these routes are selected with a mixed integer linear program. After being validated on two special cases in the literature, the matheuristic is applied to real instances in three different areas in France. Several managerial results are derived. In particular, it is found that the amount of cost reduction induced by the people assignment is equivalent to the amount of cost reduction induced by the sharing of vehicles between institutions.
This is a preview of subscription content, log in via an institution to check access.
Access this article
Price includes VAT (Russian Federation)
Instant access to the full article PDF.
Rent this article via DeepDyve
Institutional subscriptions
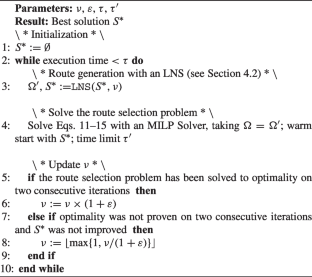
Similar content being viewed by others
Dynamic programming based metaheuristics for the dial-a-ride problem.
Ulrike Ritzinger, Jakob Puchinger & Richard F. Hartl

An ALNS algorithm for the static dial-a-ride problem with ride and waiting time minimization
Christian Pfeiffer & Arne Schulz

Typology and literature review for dial-a-ride problems
Yves Molenbruch, Kris Braekers & An Caris
Mosquera Varela AF, Trilling L, Monteiro T (2017) Managing the accompanying path of people with disabilities in a medico-social network: a method to create a process model based on autonomous actors point of views. In: 20th IFAC World congress of the international federation of automatic control (IFAC 2017)
Tellez O, Daguet L, Lehuédé F, Monteiro T, Osorio Montoya G, Péton O, Vercraene S (2020) A stakeholder oriented approach to the optimization of transports of people with disabilities. Supply Chain Forum: An Int J 21(2):93–102
Article Google Scholar
Gonzalez L, Roussel R, Héam J-C, Mikou MC (2017) Health expenditure in 2017 - results of the health accounts - 2018 ed. (fr: Les dépenses de santé en 2017 - résultats des comptes de la santé - Édition 2018.). Technical report, Direction de la recherche, des études, de l’évaluation et des statistiques. https://drees.solidarites-sante.gouv.fr/publications/panoramas-de-la-drees/les-depenses-de-sante-en-2017-resultats-des-comptes-de-la-sante
Lesteven P, Robert E, Wahl T, Grimonprez PE (2016) Health transportation - 2016 expenditure review (fr: Les transports sanitaires - revue de dépenses 2016.). Technical report, Inspection générale des affaires sociales (IGAS). https://www.igas.gouv.fr/spip.php?article557 . Accessed 1 Oct 2023
ANAP (2016) Transport - improving the management of transport for disabled people - volume 1: Feedback (fr: Transports - améliorer la gestion des transports de personnes handicapées - tome 1 : Retour d’expériences). Technical report, ANAP. https://ressources.anap.fr/transports/publication/2426 . Accessed 1 Oct 2023
Braekers K, Kovacs AA (2016) A multi-period dial-a-ride problem with driver consistency. Transp Res B Methodol 94:355–377
Tellez O, Vercraene S, Lehuédé F, Péton O, Monteiro T (2022) The time-consistent dial-a-ride problem. Networks 79(4):452–478. https://doi.org/10.1002/net.22063 , eprint: https://onlinelibrary.wiley.com/doi/pdf/10.1002/net.22063 . Accessed 09 Jan 2023
Lindstrøm C, Røpke S (2022) Group consistent dial-a-ride using adaptive large neighborhood search: 13th International conference on computational logistics
Tellez Sanchez OA (2019) Optimizing the daily transport for people with disabilities. PhD thesis, Université de Lyon, INSA Lyon. 2019LYSEI059. http://www.theses.fr/2019LYSEI059/document . Accessed 1 Oct 2023
Qu Y, Bard JF (2013) The heterogeneous pickup and delivery problem with configurable vehicle capacity. Transp Res Part C: Emerg Technol 32:1–20
Tellez O, Vercraene S, Lehuédé F, Péton O, Monteiro T (2018) The fleet size and mix dial-a-ride problem with reconfigurable vehicle capacity. Transp Res Part C: Emerg Technol 91:99–123
Genet N, Boerma WG, Kringos DS, Bouman A, Francke AL, Fagerström C, Melchiorre MG, Greco C, Devillé W (2011) Home care in Europe: a systematic literature review. BMC Health Serv Res 11(1):207
Mankowska DS, Meisel F, Bierwirth C (2014) The home health care routing and scheduling problem with interdependent services. Health Care Manag Sci 17(1):15–30
Malagodi L, Lanzarone E, Matta A (2021) Home care vehicle routing problem with chargeable overtime and strict and soft preference matching. Health Care Manag Sci 24(1):140–159
Kelle P, Woosley J, Schneider H (2012) Pharmaceutical supply chain specifics and inventory solutions for a hospital case. Oper Res Health Care 1(2):54–63
Uthayakumar R, Priyan S (2013) Pharmaceutical supply chain and inventory management strategies: Optimization for a pharmaceutical company and a hospital. Oper Res Health Care 2(3):52–64
Coster JE, Turner JK, Bradbury D, Cantrell A (2017) Why Do People Choose Emergency and Urgent Care Services? A Rapid Review Utilizing a Systematic Literature Search and Narrative Synthesis. Academic Emerg Med: Official J Soc Academic Emerg Med 24(9):1137–1149
Li M, Vanberkel P, Carter AJE (2019) A review on ambulance offload delay literature. Health Care Manag Sci 22(4):658–675
Mahon AGM (2011) Non-emergency patient transport: an integral part of accessible comprehensive health care. SAMJ: South African Med J 101(10):684–685 .Publisher: South African Medical Association
Huggins C, Shugg D (2008) Non-Emergency Patient Transport in Victoria: An overview. Australasian J Paramedicine 6(4). Number: 4
Fogue M, Sanguesa JA, Naranjo F, Gallardo J, Garrido P, Martinez FJ (2016) Non-emergency patient transport services planning through genetic algorithms. Expert Syst Appl 61:262–271
Qu Y, Bard JF (2015) A Branch-and-Price-and-Cut Algorithm for Heterogeneous Pickup and Delivery Problems with Configurable Vehicle Capacity. Transportation Science 49(2):254–270. Publisher: INFORMS
Feillet D, Garaix T, Lehuédé F, Péton O, Quadri D (2014) A new consistent vehicle routing problem for the transportation of people with disabilities. Networks 63(3):211–224
Tellez O, Vercraene S, Lehuédé F, Péton O, Monteiro T (2021) The time-consistent dial-a-ride problem. Networks 22063
Hains IM, Marks A, Georgiou A, Westbrook JI (2011) Non-emergency patient transport: what are the quality and safety issues? A systematic review. Int J Quality in Health Care: J Int Soc Quality in Health Care 23(1):68–75
Worrall P, Chaussalet TJ (2015) A structured review of long-term care demand modelling. Health Care Manag Sci 18(2):173–194
Cordeau J-F, Laporte G (2003) A tabu search heuristic for the static multi-vehicle dial-a-ride problem. Transp Res B Methodol 37(6):579–594
Molenbruch Y, Braekers K, Caris A (2017) Typology and literature review for dial-a-ride problems. Ann Oper Res 259(1):295–325
Ho SC, Szeto WY, Kuo Y-H, Leung JMY, Petering M, Tou TWH (2018) A survey of dial-a-ride problems: Literature review and recent developments. Transp Res B Methodol 111:395–421
Lehuédé F, Masson R, Parragh SN, Péton O, Tricoire F (2014) A multi-criteria large neighbourhood search for the transportation of disabled people. J Oper Res Soc 65(7):983–1000
Parragh SN (2011) Introducing heterogeneous users and vehicles into models and algorithms for the dial-a-ride problem. Transp Res Part C: Emerg Technol 19(5):912–930
Masson R, Lehuédé F, Péton O (2014) The dial-a-ride problem with transfers. Computers & Operations Research 41:12–23
Braekers K, Caris A, Janssens GK (2014) Exact and meta-heuristic approach for a general heterogeneous dial-a-ride problem with multiple depots. Transp Res B Methodol 67:166–186
Malheiros I, Ramalho R, Passeti B, Bulhões T, Subramanian A (2021) A hybrid algorithm for the multi-depot heterogeneous dial-a-ride problem. Computers & Operations Research 129:105196
Ghiani G, Improta G (2000) An efficient transformation of the generalized vehicle routing problem. Eur J Oper Res 122(1):11–17
Moccia L, Cordeau J-F, Laporte G (2012) An incremental tabu search heuristic for the generalized vehicle routing problem with time windows. J Oper Res Soc 63(2):232–244
Dumez D, Lehuédé F, Péton O (2021) A large neighborhood search approach to the vehicle routing problem with delivery options. Transp Res B Methodol 144:103–132
Dumez D, Tilk C, Irnich S, Lehuédé F, Péton O (2021) Hybridizing large neighborhood search and exact methods for generalized vehicle routing problems with time windows. EURO J Transp Logistics 10:100040
Pinson C, Afsar HM, Prodhon C (2016) Heuristic approaches to solve a generalized dial-a-ride problem applied to car-pooling. IFAC-PapersOnLine 49(12):1187–1191
Osorio G, Monteiro T, Trilling L, Albert F (2017) Multi-criteria assignment policies to improve global effectiveness of medico-social service sector. Eng Appl Artif Intell 61:21–34
Pisinger D, Ropke S (2007) A general heuristic for vehicle routing problems. Computers & Operations Research 34(8):2403–2435
Gschwind T, Drexl M (2019) Adaptive Large Neighborhood Search with a Constant-Time Feasibility Test for the Dial-a-Ride Problem. Transp Sci 53(2):480–491
Parragh SN, Schmid V (2013) Hybrid column generation and large neighborhood search for the dial-a-ride problem. Computers & Operations Research 40(1):490–497
Dueck G (1993) New Optimization Heuristics: The Great Deluge Algorithm and the Record-to-Record Travel. J Comput Phys 104(1):86–92
Mapotempo (2023) Mapotempo - Route Planning | Route Optimization | Live Tracking. https://www.mapotempo.com/ . Accessed 1 Oct 2023
Download references
Acknowledgements
For the purpose of Open Access, a CC-BY public copyright license has been applied by the authors to the present document and will be applied to all subsequent versions up to the Author Accepted Manuscript arising from this submission.
Author information
Authors and affiliations.
Univ Lyon, INSA Lyon, Université Claude Bernard Lyon 1, Univ Lyon 2, DISP-UR4570, 21 avenue Jean Capelle, Villeurbanne, 69621, Auvergne Rhone-Alpes, France
Chane-Haï Timothée, Vercraene Samuel & Monteiro Thibaud
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Monteiro Thibaud .
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix: BKS Section 6.1
Rights and permissions.
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Reprints and permissions
About this article
Timothée, CH., Samuel, V. & Thibaud, M. The assignment-dial-a-ride-problem. Health Care Manag Sci 26 , 770–784 (2023). https://doi.org/10.1007/s10729-023-09655-2
Download citation
Received : 09 November 2022
Accepted : 06 September 2023
Published : 21 October 2023
Issue Date : December 2023
DOI : https://doi.org/10.1007/s10729-023-09655-2
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Health care operations management
- Sanitary transportation
- Dial-a-ride
- Matheuristic
- Large neighborhood search
- Operations research
- Optimization
- Find a journal
- Publish with us
- Track your research
Why making your problem child an ambassador might merit a second thought

Pope Francis meets Archbishop Georg Gänswein, personal secretary to the late Pope Benedict XVI, in the library of the Apostolic Palace at the Vatican May 19, 2023. (Credit: Vatican Media.)
ROME – Rumors set in motion this week by a journalist close to Pope Francis, Elisabetta Piqué of Argentina’s La Nacion , suggest the pontiff may be on the verge of naming his erstwhile bête noire , German Archbishop Georg Gänswein, as his apostolic nuncio, meaning ambassador, to an unspecified foreign country.
Yesterday, veteran Vatican writer Gian Guido Vecchi of Corriere della Sera speculated that the assignment might be to the Baltic states of Lithuania, Estonia and Latvia, a post vacant since March 11 when Archbishop Petar Rajič, the previous occupant, was named the new papal envoy to Italy and San Marino.
The reports come in the wake of well-documented tensions between Francis and Gänswein, in the latter’s role as the top aide to the late Pope Benedict XVI – “well-documented,” in large part, because both men have spoken remarkably openly of their rifts in tell-all books written in collaboration with reporters. Ganswein did so in Nient’altro che le verità (“Nothing but the Truth”) with Italian journalist Saverio Gaeta, and Francis replied in El sucesor (“The Successor”) with Spanish journalist Javier Martínez-Brocal.
Among admirers of Pope Francis, the possibility of giving Gänswein a new gig, after exiling him back to Germany after Benedict’s death with nothing to do, is being spun as a laudable choice to let bygones be bygones. As Piqué phrased it in her April 10 piece, it would be “an unexpected decision, but totally in line with that mercy, openness of heart and lack of rigidity that the first Jesuit pope has preached since the beginning of his pontificate.”
Those less inclined to see Francis in such glowing terms may be tempted to style it instead as a hollow PR move, intended to take the edge off the pontiff’s rather intemperate criticism of Gänswein in the new book, saying he lacked “nobility and humanity,” without actually affording him much real influence or authority, and notably placing him far away from the action in Rome.
(An editorial cartoon in Corriere della Sera on Sunday showed Gänswein with his bags packed under the caption, “Before, I was in the Vatican. Now they’re sending me to Lithuania and saying it’s a sign of closing the gap with the pope. Really??”)
Yet even setting aside the subjective question of the pope’s intent, there are a couple of structural reasons why naming Gänswein a papal ambassador under the present circumstances might merit a second thought.
Before coming to that, let’s dismiss one potential objection, which is that the 67-year-old Gänswein did not study at the Pontifical Ecclesiastical Academy, the usual training ground for future papal envoys, and has no diplomatic experience, and therefore arguably might be unqualified.
First of all, there’s precedent for a former official of the Vatican’s doctrinal office successfully transitioning into the Vatican’s diplomatic service: American Archbishop Charles Brown, who served in the Congregation for the Doctrine of the Faith from 1994 to 2011, when Pope Benedict XVI named him his envoy to Ireland. By all accounts, Brown did a creditable job helping the Irish church navigate the tempests of the sexual abuse crisis, and today is serving as the apostolic nuncio to the Philippines.
Having held the post of Prefect of the Papal Household under both Benedict and Francis, Gänswein is adept at dealing with heads of state and other diplomatic actors, and almost certainly could figure out whatever else he needs to know fairly quickly.
The real objections to such a nomination have to do with what it says about the country to which Gänswein might be assigned, and also about the role of an apostolic nuncio itself.
To begin with the country, the most important thing any nation cares about when one of its diplomatic partners is picking a new ambassador is whether the choice indicates they’re being taken seriously. Assign someone perceived to have real heft with the administration he or she represents, and the receiving country will feel positive about the pick; select someone perceived as an outsider – or, worse, someone seen as being in disfavor with his or her boss – and the appointment could come across almost as an insult.
It’s almost tantamount to saying, “I care so little about our relationship with you that I’m sending you somebody I don’t really trust, just to get him out of the way.”
As a corollary, such perceptions would also likely limit Gänswein’s effectiveness. The most important asset any ambassador has is the perception that he or she can speak authoritatively on behalf of their boss. Under these circumstances, however, it seems reasonable that a host nation to might have their doubts about how seriously to take whatever Gänswein says as a statement of papal intentions.
In addition, there’s also the matter of the impact of such an appointment on the morale of the Vatican diplomatic corps.
Over the centuries, serving as a papal envoy has been seen as a tremendously important role, with Rome’s A ccademia , founded by Pope Clement XI in 1701 to train papal diplomats, traditionally seen as a “cream of the crop” destination for young clerics. Nuncios are not only the voice and face of the pope in exchanges which the governments to which they’re accredited, but they also represent the Holy See and the pontiff in the life of the local church in that country.
In other words, it’s a critical posting, and any pope should want the people charged with such a responsibility to take it seriously.
Given that, one might reasonably ask whether it’s wise for any pope to send the signal, however inadvertently, that he cares so little about the nuncio’s role that he’s willing to burn a spot simply to get rid of a figure perceived as a problem.
To come back to the comparison with Brown, when he was dispatched to Ireland in 2011, it was perceived that he came with the pontiff’s deep trust and personal support, and he was stepping into a situation where his background with the canonical dimension of the abuse crisis would be uniquely helpful. The fact Brown was an outsider to the diplomatic world thus wasn’t taken by other nuncios as a slight, but it’s hard to see how they would draw the same conclusion about Gänswein.
None of this, of course, is to suggest that Pope Francis doesn’t genuinely want to bury the hatchet, or that he doesn’t believe Gänswein could acquit himself well as an ambassador. It does suggest, however, that if the idea moves forward, the pontiff may want to find some way to make clear that this is more than what the Italians derisively call a parcheggio , meaning a parking spot, just to give Gänswein something to do.
Otherwise, for the sake of solving a temporary headache, the pope may end up with longer-term problems, both with another country and within his own diplomatic corps.
For the cost of a cup of coffee at Starbucks, you can help keep the lights on at Crux.

Tuesdays on

Crux . Anytime . Anywhere .
Today’s top stories delivered straight into your inbox.

The Lord Jesus shows us by his holy life how we are to pray

For Popes, meeting the press has always been risky business
- John L. Allen Jr.

Pope’s ‘white flag’ ironically sparks political civil war in Italy

Pope’s global round-up interesting in part for what he didn’t say

80 years ago today, a priest who incarnated the ‘social gospel’ was martyred

- Father Jeffrey F. Kirby

Pope lends support to Peru farmers claiming harassment by Catholic group
- Elise Ann Allen

New study expresses ‘grave concerns’ over definition of ‘brain death’
- Charles Collins

Pope Francis to visit Asia and Oceania in September
- Nirmala Carvalho
IMAGES
VIDEO
COMMENTS
For our study, the assignment cost c ij between patient i and doctor j refers to the related costs that are involved in preparing, operating, and managing the telemedicine assignment by the medical center (e.g., NTCC) in practice, which seems to be commonly used in the classical healthcare assignment literature (e.g., Zhang et al., 2018a, Wang ...
This research work investigates the well-researched nurse scheduling problem with proposing a variable time quantum based nurse assignment. It opens up various problems and solutions in assigning nurses to patients in required shift patterns on the basis of their appropriate expertise and grade with severity of the patients in any hospital, nursing centre or in remote healthcare services every ...
However, the development of such systems [22,23,24,25] is contingent upon the successful resolution of the patient assignment (PA) problem. The PA problem is a crucial aspect of cloud healthcare systems, as it directly impacts the efficiency and effectiveness of the system.
To address these challenges, in this paper, we developed a mixed-integer linear programming (MILP) model employing the Gurobi optimization solver. The model includes staff assignments, patient assignments, resource allocations, and overtime hours to minimize healthcare expenditures and enhance patient care.
Abstract and Figures. The nurse-to-patient assignment problem in Home Care (HC) under continuity of care consists of allocating each newly admitted patient to only one reference nurse, without ...
The Gurobi solver's powerful optimization algorithms can address challenging healthcare problems, including resource allocation, staffing, and patient assignment. ... Grunder, O. A matheuristic approach to the integration of worker assignment and vehicle routing problems: Application to home healthcare scheduling. Expert Syst. Appl. 2019, 125 ...
This paper proposes a data-driven method to estimate the travel times of care givers in the assignment problem when their routes are not available yet, and results indicate that the proposed estimation method performs better than the average value and k-nearest neighbor search methods. Abstract Home health care is one of the recent service systems where human resource planning has a great ...
The planning process of interest developed in this paper is deciding which operator is in charge of which customers, i.e. the assignment problem. Home health care (HHC) is an example of such mobile services that has known a fast recent growth in the health care sector, representing an alternative to the conventional hospitalization in developed ...
problems, including resource allocation, staffing, and patient assignment. These findings suggest that healthcare professionals may boost efficiency and quality .
Critical thinking/problem-solving skills should emphasize self-examination. It should teach an individual to accomplish this using a series of steps that progress in a logical fashion, stressing that critical thinking is a progression of logical thought, not an unguided process. Pedagogy.
Abstract. This paper studies a Multidimensional Assignment Problem (MAP) applied in the medical sector. The case study is taken from a major french medical service provider. This problem consists of assigning medical employees to perform healthcare or administrative tasks at workplaces within a predefined scheduling horizon.
Here's how it works: Medicare will pay the provider 95% of the amount they would pay if the provider accepted assignment. The provider can charge the person receiving care more than the Medicare-approved amount, but only up to 15% more (some states limit this further). This extra amount, which the patient has to pay out-of-pocket, is known as ...
There are 4 modules in this course. In this course, we're going to go over analytical solutions to common healthcare problems. I will review these business problems and you'll build out various data structures to organize your data. We'll then explore ways to group data and categorize medical codes into analytical categories.
Finding and choosing a strong research topic is the critical first step when it comes to crafting a high-quality dissertation, thesis or research project. If you've landed on this post, chances are you're looking for a healthcare-related research topic, but aren't sure where to start. Here, we'll explore a variety of healthcare-related research ideas and topic thought-starters across a ...
1. Financial difficulties. In 2023, health systems will likely continue to face financial difficulties due to ongoing staffing problems, reduced patient volumes, and rising inflation. According to Tina Wheeler, U.S. health care leader at Deloitte, hospitals can expect wage growth to continue to increase even as they try to contain labor costs.
Assigning inpatients to hospital beds impacts patient satisfaction and the workload of nurses and doctors. The assignment is subject to unknown inpatient arrivals, in particular for emergency patients. Hospitals, therefore, need to deal with uncertainty on actual bed requirements and potential shortage situations as bed capacities are limited. This paper develops a model and solution approach ...
Technological Innovation in Health Care . Technological innovation in health care can be disruptive, consumer-driven, or focused on improving the business model. In many cases, new technology innovates in all of these ways. Some of the most recent technologies have drastically improved health care in exciting and often awe-inspiring ways.
A report from the Department of Health and Human Services' inspector general finds a dire shortage of mental health care providers in Medicaid and Medicare, which together serve some 40% of Americans.
In this work, the therapist assignment problem (TAP) is described from two perspectives, that is, patient and therapist or demand and supply. A patient demand is categorized on the basis of the different PP and COC levels, which are related to pathologies and that patient's eagerness to the COC. A therapist supply is classified according to the ...
NPR's Scott Simon speaks with Jennifer Erickson, senior fellow with the Federation of American Scientists, about the organ transplant system and how eligible donated organs wind up in the trash.
Your health care team may be able to recommend other resources, such as a healthy lifestyle coach, to help you with making changes. Ask your health care team or your insurance company if your benefits include medical nutrition therapy or other diabetes care resources. Talk with your health care professional before taking dietary supplements
A cyberattack earlier this year on Change Healthcare, which operates the largest clearinghouse for medical claims in the U.S., destabilized the country's healthcare system, halting billions of ...
In healthcare scheduling problems many problems receive less attention by researchers, in this section will surveyed and give an overview of other healthcare scheduling such as scheduling physicians [123,124,125], home healthcare [126,127,128], telemedicine scheduling . Physician scheduling is a real-world problem which arises in hospitals ...
We deal with a Home Health Care Problem (HHCP) which objective consists in constructing the optimal routes and rosters for the health care staffs. ... The assignment problem we solve is defined as follows: (P ) min âˆ' i,j∈S ′′ (D i + d ij + W ij )x ij s.t. âˆ' i∈S ′′ x ij = 1 ∀j ∈ S â ...
Attempts to gain power partially fueled Arizona's abortion ban in 1864. Male physicians sought to dominate health care, and xenophobic fears about immigrants emerged, historians said.
In this paper, we present the first Assignment-Dial-A-Ride problem motivated by a real-life problem faced by medico-social institutions in France. Every day, disabled people use ride-sharing services to go to an appropriate institution where they receive personal care. These institutions have to manage their staff to meet the demands of the people they receive. They have to solve three ...
Among admirers of Pope Francis, giving Gänswein a new gig, after having dispatched him back to Germany after Benedict's death with no assignment at all, is being spun as a laudable decision to ...
A branch-and-price method for a tactical assignment problem in healthcare is proposed. • The approach maximizes the minimum service level across all blocks of time. • In some cases the service level can be greatly improved with only minimal changes. • An optimal schedule can show a robust performance when lab capacity is decreased.