- Get involved


Public Service 2030
August 27, 2018.
The UNDP’s commitment to public service excellence lies in a strong belief that those states which invest in their administrative capacities are more likely to deliver on the 2030 Agenda for Sustainable Development. With this end in mind, the UNDP Global Centre for Public Service Excellence (GCPSE) published 17 case studies, with each one focused on a different SDG.
The SDGs ultimately aim to end poverty, protect the planet, and provide a prosperous future for all. The case studies feature 17 different countries, detailing the progress made in each of the 17 SDGs (one Goal per country). In doing so, the cases illustrate the critical role the public sector played in making progress on the SDG in each country.
Personal accounts by individuals from countries including Cambodia, Libya, Papua New Guinea, Samoa, and others provide inspiring examples of how public service excellence can transform lives. Collaborative efforts between the public sector, private sector, and civil society in many of the stories are timely reminders that close partnerships will be required to achieve the Agenda 2030.
Document Type
Related publications.

Publications
Small island digital states: how digital can catalyse sid....
This major publication serves as a roadmap for Small Island Developing States policymakers, decision-makers, and innovators. It advocates for an inclusive digit...

The CAP Financial Innovation Challenge: A Summary Report ...
The report, part of the UNDP's Climate Aggregation Platform (CAP) report series published on January 26, 2024, provides an overview of the seven financial innov...

No Soft Landing for Developing Economies
Many developing economies are stuck in a negative debt-development feedback loop keeping them from undertaking new growth- and welfare-enhancing investments. Fo...

Institutionalising SDG Localization in Multi-Level Govern...
This brief presents successes and challenges from India’s SDG localization model, framed around four key insights that can inform efforts elsewhere to support t...

Gender Equality, Women's Empowerment, and Leadership in N...
This publication provides seven entry points for mainstreaming gender into planning, monitoring, and reporting for revised or updated National Biodiversity Stra...

Financial Aggregation for Distributed Renewable Energy in...
This report series seeks to demystify financial aggregation and raise awareness about its potential to enable investments in Distributed Renewable Energy (DRE) ...
- Tools and Resources
- Customer Services
- Contentious Politics and Political Violence
- Governance/Political Change
- Groups and Identities
- History and Politics
- International Political Economy
- Policy, Administration, and Bureaucracy
- Political Anthropology
- Political Behavior
- Political Communication
- Political Economy
- Political Institutions
- Political Philosophy
- Political Psychology
- Political Sociology
- Political Values, Beliefs, and Ideologies
- Politics, Law, Judiciary
- Post Modern/Critical Politics
- Public Opinion
- Qualitative Political Methodology
- Quantitative Political Methodology
- World Politics
- Share This Facebook LinkedIn Twitter
Article contents
Qualitative research and case studies in public administration.
- Jason L. Jensen Jason L. Jensen Institute of Policy and Business Analytics, University of North Dakota
- and Laura C. Hand Laura C. Hand College of Business and Public Administration, University of North Dakota
- https://doi.org/10.1093/acrefore/9780190228637.013.1747
- Published online: 29 November 2021
Public administration has experienced academic growing pains and longstanding debates related to its identity as a social and administrative science. The field’s evolution toward a narrow definition of empiricism through quantitative measurement has limited knowledge cumulation. Because the goal of all scientific endeavors is to advance by building upon and aggregating knowledge across studies, a field-level point of view eschewing traditional dichotomies such as qualitative/quantitative debates in favor of methodological pluralism allows for examination of both the art and science of public administration.
To accomplish this, traditional notions of quality, namely rigor, must be reconceptualized in a way that is appropriate for the philosophical commitments of a selected methodology. Rigor should focus on the accuracy, exhaustiveness, and systematicity of data collection and analysis. This allows for quality judgments about the degree to which the methods resulted in evidence that addresses the research questions and supports stated conclusions. This is a much broader approach to rigor that addresses multiple types of inquiry and knowledge creation. Once the question of rigor is not limiting the types of research done in the field, attention can be turned to the ways in which high-quality studies can contribute to knowledge cumulation.
Case studies can be used as an example of a field-level point of view, as they have the ability to utilize abductive reasoning to consider both the whole (the entire case) and the particular (factors that contribute to outcomes, processes, or theories). Case studies explore the relationship between context-independent theories and context-dependent factors using different types of data collection and analysis: a triangulation of sorts. They can test theories in multiple ways and create or suggest new theories. Considering field-level questions as a case study and synthesizing findings from multiple related studies, regardless of methodology, can help move the field forward in terms of its connection between theory and practice, art and science.
- methodological pluralism
- case studies
- qualitative methods
- metasynthesis
- public administration and policy
You do not currently have access to this article
Please login to access the full content.
Access to the full content requires a subscription
Printed from Oxford Research Encyclopedias, Politics. Under the terms of the licence agreement, an individual user may print out a single article for personal use (for details see Privacy Policy and Legal Notice).
date: 07 April 2024
- Cookie Policy
- Privacy Policy
- Legal Notice
- Accessibility
- [66.249.64.20|185.39.149.46]
- 185.39.149.46
Character limit 500 /500
- Partnership for Public Service
- Best Places to Work
- Center for Presidential Transition
- Go Government
- Service to America Medals
- Overview and Strategy
- Board and History
- Diversity, Equity and Inclusion
- Work with Us
- Our Supporters
- Our Solutions
- Roadmap for Renewing our Federal Government
- Customer Experience
- Employee Engagement
- Innovation and Technology Modernization
- Leadership and Collaboration
- Presidential Transition
- Rebuilding Trust in Government
- Recognition
- Performance Measures
- Agency Performance Dashboard
- Best Places to Work in the Federal Government®
- Fed Figures
- Leadership 360 Assessment
- Political Appointee Tracker
- Trust in Government Dashboard
- Public Service Leadership Institute®
Public Service Leadership Model
- Leadership Training
- Read, Watch and Listen
- Latest Releases
- Search this site
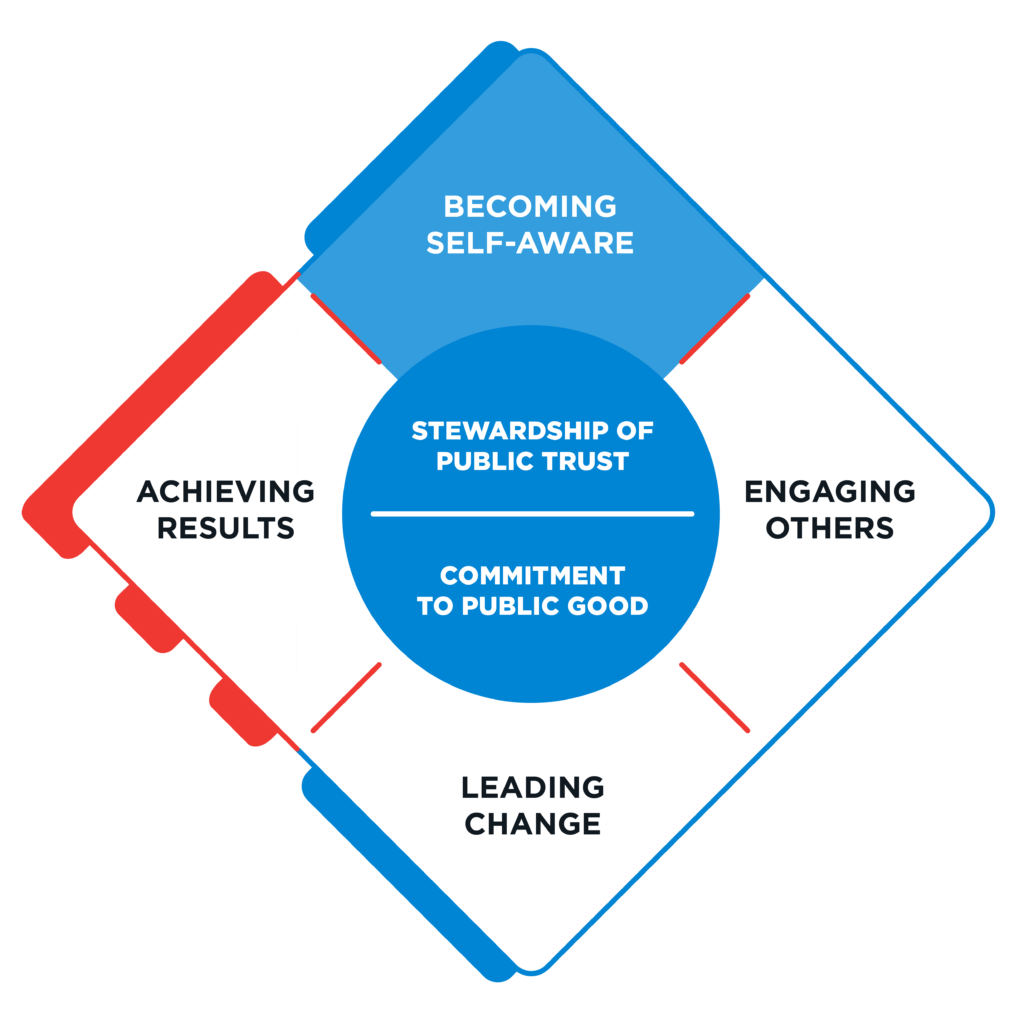
Becoming Self-Aware
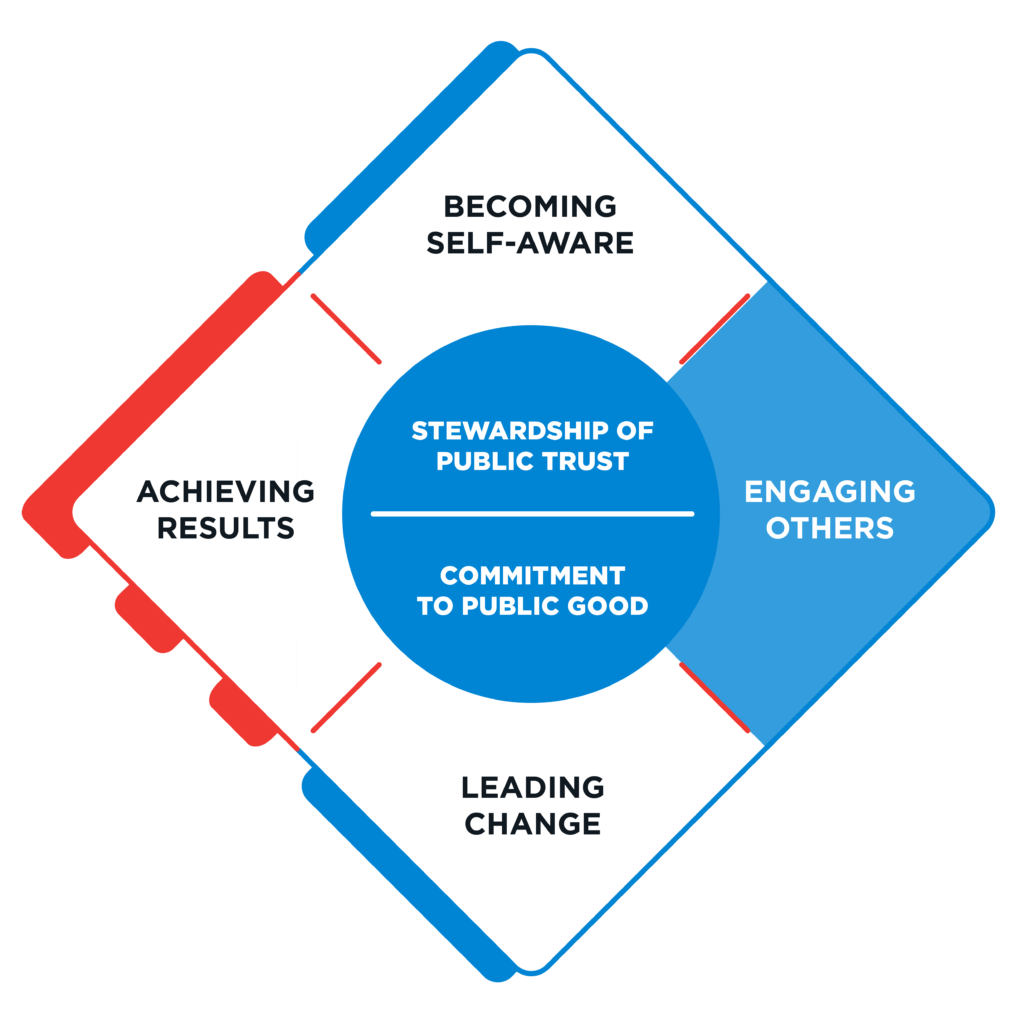
Engaging Others
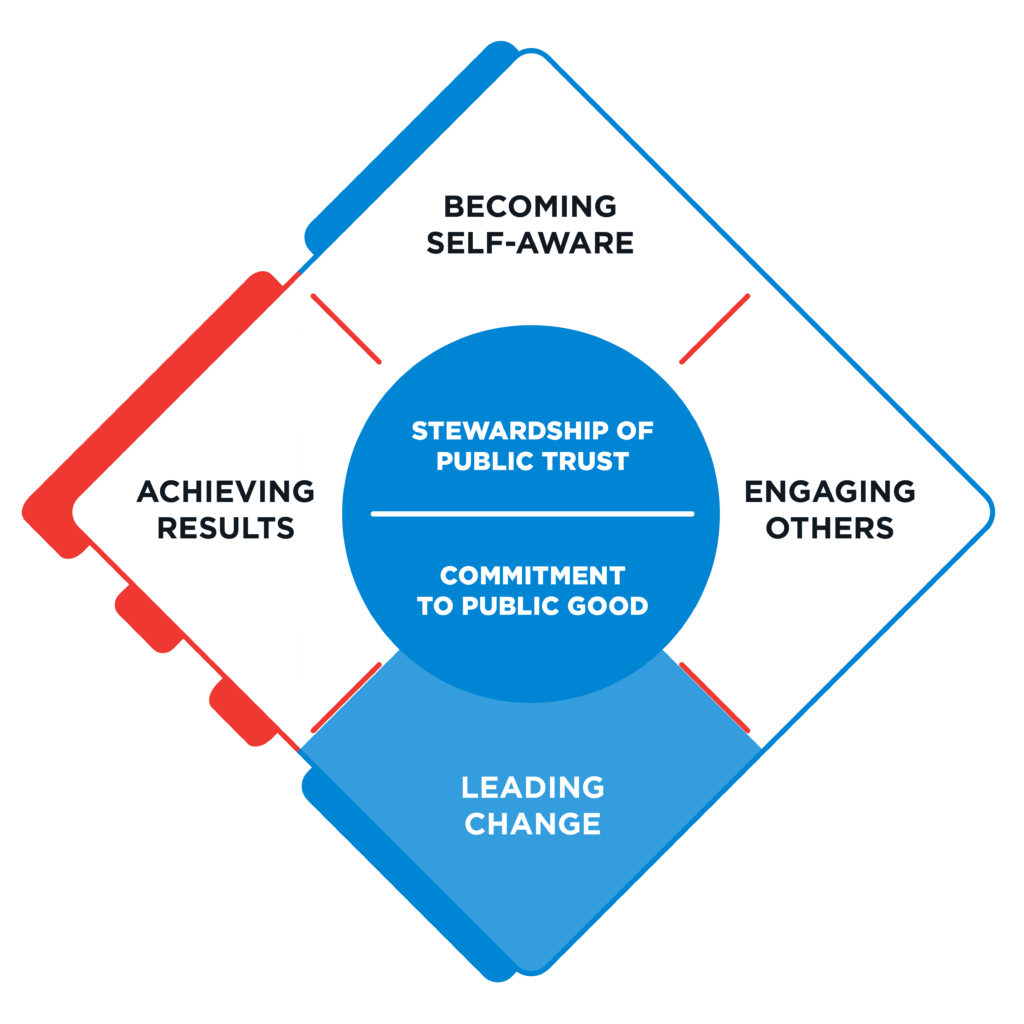
Leading Change
Achieving Results
- Core Values
The standard for effective federal leadership
Public servants aren’t driven by a financial bottom line—they’re driven by impact. Instead of asking how they can generate the biggest profits, they ask themselves, “How can we do the most good?”
That’s why we developed the Public Service Leadership Model, the standard for effective federal leadership. The model identifies the four core values leaders must prioritize, and the critical competencies they must demonstrate, to achieve their agencies’ missions and desired impact. By using the model, leaders can evaluate their performance, assess their leadership progress and chart a course for self-improvement.

The model identifies four key leadership competencies—and several sub competencies— federal leaders need to grasp to best serve our country in the 21st century. The four competencies align with and supplement the Office of Personnel Management’s Executive Core Qualifications, providing leaders with a clear guide to address government’s current and future challenges.
Leaders can use the model as a guide to steer their growth and make decisions at different stages of their careers. Agencies can use the model as a standard for building and measuring overall leadership effectiveness.
Four key leadership competencies
Becoming self-aware begins with an understanding of your values, thought patterns and motivations. Being reflective in this way is essential to better interactions.
When engaging others, leaders foster a culture that encourages team members to offer feedback, recognize good work and pursue professional development.
Leading change in a federal environment means initiating, sponsoring and implementing innovative solutions. Leaders also help others be successful.
Achieving results means managing skillfully, thinking strategically and making good decisions that deliver measurable outcomes.
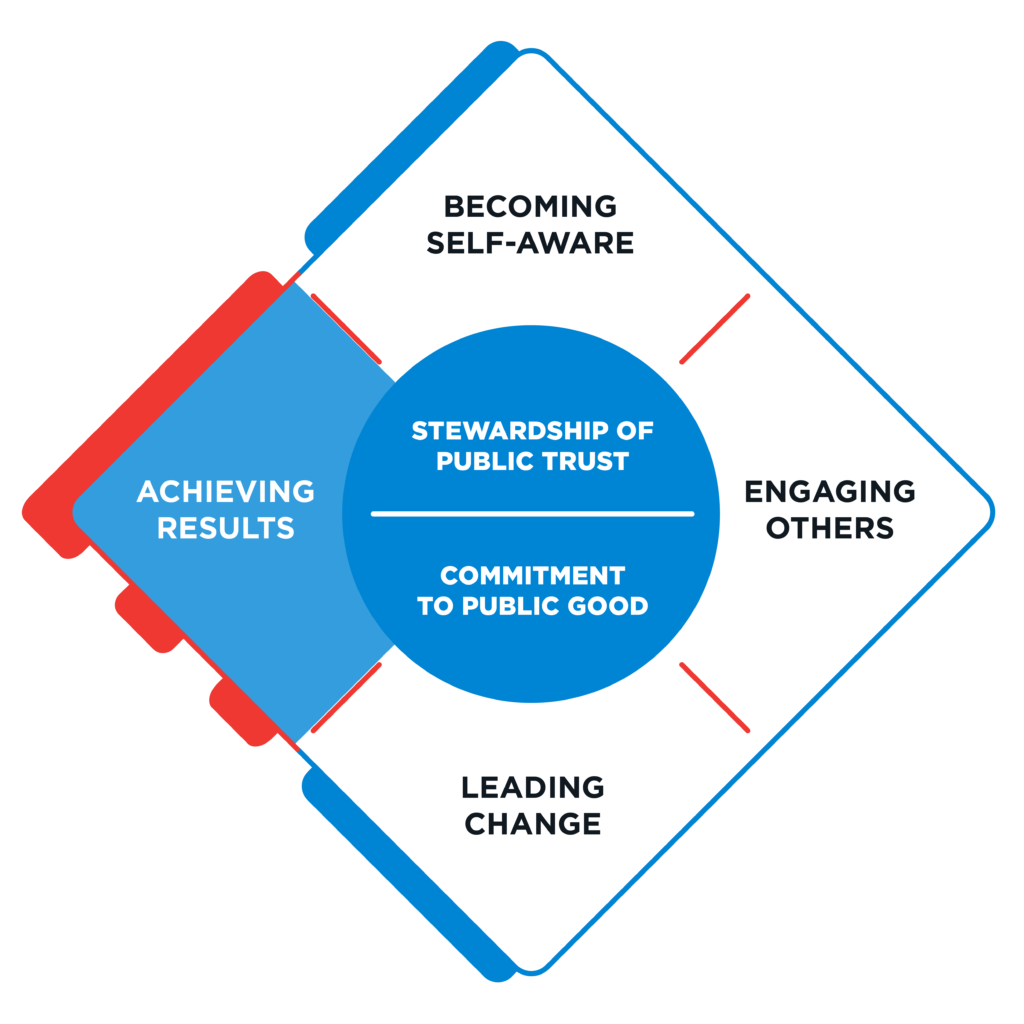
The Core Values of Government Leadership
When federal employees enter public service, they swear an oath to support and defend the Constitution. This oath serves as a true north for federal leaders who serve the American people.
Federal leaders should emulate two core values, each uniquely relevant to government, to live up to the highest ideals of public service.
Stewardship of Public Trust
Given the vast influence, power and resources of our government, trust in federal leaders and their integrity is paramount. Federal leaders represent the public and must be held to the highest standards. They are stewards of the Constitution, taxpayer dollars and the workforces they lead.
Commitment to Public Good
For federal leaders to achieve their agencies’ expansive missions and promote the general welfare, they need a deep-rooted belief in the value of public service and a strong commitment to the public good.
Types of Government Leaders by Role
Each leadership competency is critical for all government leaders—but leaders will apply them differently depending on their role and rank within their agencies. These competencies apply to supervisors and technical experts alike.
Click on a role below to learn about its competencies.
© 2023 Partnership for Public Service, Inc. All rights reserved.

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- v.10(1); 2020
Original research
The effect of leadership on public service motivation: a multiple embedded case study in morocco, zakaria belrhiti.
1 Ecole Nationale de Sante Publique, Rabat, Morocco
2 Department of Public Health, Institute of Tropical Medicine, Antwerp, Belgium
3 Department of Gerontology, Vrije Universiteit Brussel, Brussels, Belgium
Wim Van Damme
Abdelmounim belalia, bruno marchal, associated data.
bmjopen-2019-033010supp001.pdf
bmjopen-2019-033010supp002.pdf
bmjopen-2019-033010supp003.pdf
We aimed at exploring the underlying mechanisms and contextual conditions by which leadership may influence ‘public service motivation’ of health providers in Moroccan hospitals.
We used the realist evaluation (RE) approach in the following steps: eliciting the initial programme theory, designing the study, carrying out the data collection, doing the data analysis and synthesis. In practice, we adopted a multiple embedded case study design.
We used purposive sampling to select hospitals representing extreme cases displaying contrasting leadership practices and organisational performance scores using data from the Ministry of Health quality assurance programmes from 2011 to 2016.
Participants
We carried out, on average, 17 individual in-depth interviews in 4 hospitals as well as 7 focus group discussions and 8 group discussions with different cadres (administrators, nurses and doctors). We collected relevant documents (eg, performance audit, human resource availability) and carried out observations.
Comparing the Intervention-Context-Actor-Mechanism-Outcome configurations across the hospitals allowed us to confirm and refine our following programme theory: “Complex leaders, applying an appropriate mix of transactional, transformational and distributed leadership styles that fit organisational and individuals characteristics [I] can increase public service motivation, organisational commitment and extra role behaviours [O] by increasing perceived supervisor support and perceived organizational support and satisfying staff basic psychological needs [M], if the organisational culture is conducive and in the absence of perceived organisational politics [C]”.
Conclusions
In hospitals, the archetype of complex professional bureaucracies, leaders need to be able to balance between different leadership styles according to the staff’s profile, the nature of tasks and the organisational culture if they want to enhance public service motivation, intrinsic motivation and organisational commitment.
Strengths and limitations of this study
- Realist evaluation (RE) is useful in explaining how, why and under which conditions an intervention or a social phenomenon (leadership in our study) generates a particular outcome ( in casu public service motivation).
- Continuous refinement of programme theories through RE cycles allows for a cumulative process of knowledge creation by constant shuttling across cases from theory to empirical data and back.
- The time and resource constraints of the PhD research project, of which this study is a part, precludes testing and validating existing measurement scales of concepts such as public service motivation, perceived organisational support and organisational commitment.
Introduction
Health workers’ performance has received increased attention from policy makers, scholars and global health organisations, 1–3 and is recognised as an essential driver for the achievement of the sustainable development goals, 4 the implementation and the scale up of effective public health sectors reforms . 5–9
Motivation in the public sector
In low-income and middle-income countries (LMICs), poor performance of health workers is a critical barrier to quality of care and to the implementation of health policies in general. 5 10 This often stems from a lack of motivation and to negative attitudes of health workers in the provision of care. 11–15
The motivation of health workers is recognised as a critical determinant of the performance of health workers in public performance. 2 5 6 16 While staff availability, knowledge and skills are essential in health service delivery, they are not sufficient to ensure good health worker performance. This critically depends on staff motivation, and in public services specifically on their willingness to pursue public service values and work in line with the best interest of patients. 16–19
This notion is encompassed by the concept of public service motivation (PSM), understood as the altruistic desire of health workers to serve the common interest and to help patients and their families regardless of financial or external rewards. PSM has been shown to be key to the performance of public servants in public administration 20 21 and in the health sector. 22 23
Since 1990, public management scholars have been developing the concept of ‘public service motivation’ (PSM), defined as “an individual’s predisposition to respond to motives grounded primarily or uniquely in public institutions and organizations”. 24 PSM involves a set of “beliefs, values and attitudes that go beyond self-interest and organizational interest, that concern the interest of a larger political entity, and that motivate individuals to act accordingly whenever appropriate”. 25 From this perspective, health workers can be driven by an altruistic desire to serve the public interest and the population. 26–30 Research in public sector settings and in healthcare produced evidence on the positive effect of PSM on job satisfaction, reduced turnover and individual performance. 28 29 31–34 Within the field of PSM, research has focused on how managers and leaders can enhance PSM among public servants. 35–39
This perspective on the motivation offers an alternative perspective to the recent trends in health system performance management reforms inspired from new public management, including pay for performance and contracting out, which focuses on extrinsic motivation of health providers, and risks to crowd out intrinsic motivation. 30 Such strategies may also generate negative self-interested behaviours, goal displacement and mistrust. 30 40–44
Leadership in the health sector
In Morocco, research evidence points to how a lack of motivation and poor leadership of health managers may have hampered the performance of health workers, the quality of care and the scaling up of proven effective health policies 45–52 and quality assurance programmes. 53 54
In LMIC, health managers often display poor leadership practices either by avoiding getting involved, delaying decisions (laissez-faire leadership) or by overemphasising top-down controlling behaviours perceived as inefficient in the motivation of health workers. 55–59
‘Traditional’ leadership theories emphasise the importance of individual leadership and leader–employee exchange relationships. They comprise transactional leadership (where leaders focus on top down contingent rewards and sanctions) and transformational leadership (where leaders focus on inspiring staff, infusing jobs with meaning and acting as a role model). 60 Recent leadership theories emphasise the need for more complex approaches that allow for better adaptation to the complex social nature of healthcare organisations. 61–63 Complex leadership scholars highlight the multilayered nature of effective leadership, which includes information sharing, distributed leadership and support for lower level cadres. They define complex leadership as the ability of leaders in complex unpredictable situations to balance between transactional, transformational and distributed leadership so as to fit the nature of task, type of staff and organisational characteristics. 61 62 64–66
The relationship between leadership and PSM
Complex processes underlie the effect of leadership on PSM, and they are conditioned by contextual factors (professionalism, religion and family education) 67–73 and organisational factors (organisational culture 74 75 and job characteristics 28 29 ).
Most PSM research in the field of public administration relies on quantitative measures of the effect of leadership on PSM. Little attention has been paid to the mechanisms underlying this relationship in healthcare and public service settings, 16 31 33 35 37 39 76–78 and the existing studies often display methodologies challenges. 79 80 Understanding these mechanisms is valuable in the sense that it can guide health managers in developing appropriate leadership and managerial practices that reinforce organisational value systems, and foster health workers’ PSM and intrinsic motivation, and consequently their performance. 59 81–83
In response, we set out to explore the causal processes through which leadership, context and organisational attributes influence public service motivation of health workers in Moroccan hospitals. The research questions we address are as follows: (1) How does leadership influence public service motivation of health workers? and (2) Which organisational or contextual conditions underlie the effect of leadership on PSM? This study is part of a larger study on the nature and effects of leadership practices on health workers in four Moroccan hospitals.
We adopted the RE approach. 84 RE aims at identifying causal mechanisms that explain how, why and under which conditions an intervention or a social phenomenon (leadership in our study) generates a particular outcome ( in casu PSM). 84 Realists posit that causal mechanisms are generative in nature and embedded in a stratified social reality; they reside in the interplay between individuals, institutional and structural factors. 85 86
We applied the steps of the realist research cycle 85 87 to structure our study: (1) eliciting the initial programme theory, (2) designing the study, (3) carrying out the data collection, (4) analysing the data and (5) synthesis. We refer to our paper reporting on a case study of leadership for more details on the realist approach. 88
Step 1: eliciting the initial programme theory
Our scoping review of complex leadership 62 allowed us to elicit an initial programme theory (PT) on the relationship between leadership and motivation. It was further developed through a first exploratory case study (coded NHMH) (see Belrhiti et al 88 ), and this led to the initial PT that is the starting point of this study:
Complex leaders adopt an appropriate mix of transactional, transformational and distributed leadership styles that fit the mission, goals, organisational culture, nature of the tasks of the organisation and the individual characteristics of the personnel. This adaptation of leadership style enhances staff perceived supervisor support and perceived organizational support, and contributes to the satisfaction of basic psychological needs of the staff ( figure 1 ). Open in a separate window Figure 1 Programme theories. PSM, public service motivation.
As we described before, 88 the underlying theories used to build our above-mentioned programme theory rely on two mechanisms that have shown to be important in explaining the complex relationship between leadership and motivation 89–91 : (1) the satisfaction of basic psychological needs, based on self-determination theory 92 (see box 1 ), and (2) perceived supervisor support and perceived organisational support 89 90 93 (see box 2 ).
Definition of basic psychological needs
According to self-determination theory, every individual thrive to satisfy three basic psychological needs (autonomy, competence, relatedness). Autonomy corresponds to the sense of volition and willingness ones feel when undertaking specific behaviours. This allow staff to self-endorse their actions. Competence needs means the feeling self efficacy when experiencing work opportunities that allow individuals to express and use their abilities and skills. Relatedness means that staff need to feel mutual respect, consideration from others, connectedness and a sense of belonging to a social group.
Perceived organisational and supervisor support
Perceived organisational support (POS) is understood as the beliefs of health workers about the extent to which the organisation (eg, top management teams) values their efforts and their psychological well-being.
Perceived supervisor support (PSS) is identical to the former but focuses on the relationship between staff and their supervisor.
In this study, we adopted a dynamic perspective of leadership which we considered as a multilevel process embedded in a multilayered social and organisational context. 62 64 94–98 From this perspective, leadership is shaped by the organisational culture and by how staff interpret their organisational context (organisational climate). 99–101
We mean by the organisational culture “the shared values, underlying assumptions and expectations that characterise organisational membership”. 102 Different types of organisational culture are presented in box 3 . 103 The visible aspect of the organisational culture is represented by the organisational climate (‘the tip of the iceberg’) and is “the visible behaviour of group members”. 99
Types of organisational culture according to Cameron and Quinn
Hierarchical culture: strong emphasis on stability, predictability and efficiency. Formalisation, procedures and rules govern individual behaviour.
Clan culture: emphasis on cohesion, teamwork, high levels of employee morale, employee involvement and commitment within an autonomy supportive environment.
Market culture: emphasis on employee productivity, results and profit orientation, individualism and competitiveness, in an environment that is considered as hostile.
Adhocratic culture: emphasis on creativity, innovation, individuality, experimentation, risk taking and adaptability. Power is decentralised to task teams.
We adopt the definition of organisational climate of Bock e t al : the “contextual situation at a point in time and its link to the thoughts, feelings, and behaviours of organizational members. Thus, it is temporal, subjective, and often subject to direct manipulation by people with power and influence”. 104 It is a multidimensional concept that includes role conflict and ambiguity, professional and organisational esprit, job challenges, workgroup cooperation and mutual trust. 105
Figure 1 shows our programme theory (PT) and the complex relationship between leadership, individual motivation and organisational characteristics (organisational culture and climate, mission and goals, and degree of responsiveness to basic psychological needs). 88 The quality and type of staff motivation (extrinsic vs autonomous motivation, including PSM and intrinsic motivation) depends on the degree of autonomy support by leaders, and consequently their perceived supervisor support (which in itself is increased by transformational and distributed leadership and reduced by laissez-faire and transactional leadership). Autonomous motivation is enhanced when staff have positive levels of perceived organisational support, which depends on the degree of responsiveness of top management teams to staff’s basic psychological needs and the congruence between the organisational culture and the individual values.
More specifically, we identified four causal configurations ( figure 1 ):
Configuration 1
- Laissez-faire leadership decreases the levels of perceived organisational support and staff motivation by being less responsive to their basic psychological needs of autonomy, competence and relatedness. Lack of vision and goal setting contributes to a climate of ambiguity and role conflict. The inadequate enforcement of the hierarchical structure and high job pressure can contribute to mistrust between administration and staff.
Configuration 2
- Transactional leaders can improve extrinsic motivation of staff if they offer the necessary support and ensure adequate working conditions. By improving the latter, transactional leaders reduce job pressure, and by implementing a clear hierarchical line, they reduce role conflicts.
Configuration 3
- By showing individual consideration and communicating clearly about mission valence, transformational leaders enhance self-esteem of staff, perceived supervisor support and satisfaction of their autonomy needs. This in turn contributes to staff commitment, mutual trust and respect between the management team and staff.
Configuration 4
- Distributed leadership can contribute to improved communication and interaction between staff from different units, to problem solving and a reinforced clan culture. Distributing leadership roles and embedding them throughout the organisation, combined with engaging staff in decision making, contributes to staff’s perceived autonomy and organisational commitment, which in turn leads to extra role activities.
In this study, we zoom in on the role of public service motivation. We assume that leaders who stimulate staff’s awareness of the value of their work to society and its contribution to the public good may enhance PSM and intrinsic motivation. Leaders who are responsive to the basic psychological needs of their staff are likely to stimulate the internalisation of public values and may shift the locus of individual motivation from extrinsic to more autonomous forms of motivation. 106 This requires a conducive organisational culture and absence of conflicts between individual and organisational values. We hypothesise that the specific attributes of the Moroccan health system, and specifically its hierarchical organisational culture, may impede the emergence of PSM.
Step 2: study design—a multiple embedded case study design
We adopted a multiple case study design 107 because it fits the exploration of multifaceted complex phenomena, such as PSM, in real-world settings (in our case in four hospitals). We defined the case as the relationship between leadership and ‘public service motivation’. We took a hospital as the unit of analysis. Purposive sampling allowed us to select hospitals that would allow us to test the PT. We selected hospitals representing extreme cases, displaying contrasting organisational performance and leadership practices. 108 109 To select hospitals, we used data from the Ministry of Health’s quality assurance programme called ‘concours qualité’ from 2011 to 2016. 110 111 More specifically, we used the leadership scores and the overall organisational quality performance scores ( table 1 ). We refer to Sahel et al 54 for a discussion of the ‘concours qualité’.
List of high-performing and low-performing hospitals (Ministère de la santé du Maroc, 2011 and 2016 report)
We purposefully selected two well-performing hospitals with high leadership scores (NHMH and EJMH) and two poor-performing hospitals with low leadership scores (RKMH and SMBA) ( table 1 ). This selection was informed by independence of cases, variation in hospital size (seeking to have one large and one small sized hospital in each category), variation in location (urban, periurban, rural) and accessibility to the first author.
RE seeks to refine PTs through a process of specification: the PT is gradually refined by testing it in different settings or in different cases. For this study, we started the data collection in NHMH and developed a first refined PT. This was then tested in EJMH and the poor-performing hospitals RKMH and SMBA. The analysis of each site led to successive refinement, confirmation or disconfirmation of the elements of the initial PT.
Step 3: data collection
We based the choice of the data collection methods on our PT ( figure 1 ) to ensure that data would allow us to test the initial PT. We used interviews, focus group discussions and document review (see figure 2 ). We collected data during the period January–June 2018.

Case studies and data collection, Morocco, January–June 2018.
In each hospital, we interviewed health professionals, and senior, middle and operational managers. We explored the antecedents of PSM, its expression and the relationship with leadership and management practices, organisational structure and cultural context. We used open-ended interview guides tailored to each category of respondents ( online supplementary file 1 ). We collected data until saturation was attained. In the first site (NHMH), we carried out 18 individual in-depth interviews (IDIs). Subsequently, we carried out 17, 16 and 17 IDIs in EJMH, RKMH and SMBA, respectively. Each respondent was anonymised and given a unique identifier. Sociodemographic characteristics of the respondents are summarised in table 2 .
Respondent characteristics
Supplementary data
Focus group discussions.
To further explore the key constructs used by interviewees in relation to ‘public service motivation’, we carried out seven focus group discussions and eight group discussions with different cadres (administrators, nurses and doctors). Group discussions were carried out whenever the number of participants did not reach the appropriate size (six to eight) to carry out focus group discussions (FGDs). This was encountered in practice in low staffed hospitals (RKMH and NHMH) particularly for doctors and administrative staff.
This allowed us to deepen the analysis across the different categories of health workers (managers, service providers). The first author led the FGD. Probes, follow-up questions and summarised key themes were used and verification from participants was sought at the end of each FGD. 112 113 The FGD facilitator guide is presented in online supplementary file 2 .
Respondents for the IDIs and the FGDs were identified through qualitative purposive sampling. 108 All FGD and IDI were audio recorded with the exception of one interview. In this specific case, we took notes and transcribed the unrecorded interview using memory recall. 114 Following guidance provided by Miles and Huberman 115 and Krueger and Casey, 112 we wrote a brief contact summary at the end of any contact with research participants. It included major themes and ideas arising after each interaction. All recordings were transcribed verbatim. Two researchers (ZB and BM) checked the transcripts for accuracy.
Document review
We collected documents at the study sites (760 pages) and at the Ministry of Health (460 pages). We focused on human resources availability and skill mix, the strategic plans of the hospitals, audit documents and quality assurance reports.
Observations
The first author carried out opportunistic observations (between appointments with interviewee), following the guidance described by Spradley. 116 Close attention was paid to the interaction between supervisors and staff. We recorded our observations about feelings and goals expressed during informal interaction with hospital staff and external actors and the physical spaces.
Step 4: analysis
We carried out the data analysis following the ‘traditional’ analytical phases of compiling data, interpreting, discussion and drawing conclusions. 109 Guided but not restricted by the initial PT, we coded all data sources (transcripts, contact summaries and field notes) using different coding techniques (concept, hypothesis and ‘in vivo’ coding) 117 (see online supplementary file 3 ). We used the ICAMO (Intervention-Context-Actor-Mechanism-Outcome) heuristic to identify causal configurations. We revisited the data to test conjectural ICAMO configurations. 118 We adopted a retroductive approach 119 to contrast patterns of leadership effectiveness between different types of actors (doctors, nurses and administrators). We compared these patterns with the chronology of the Chief Executive Officer (CEO) succession periods. Guided by our research question, we focused on leadership effects on ‘public service motivation’ that emerged as a natural motivational driver of Moroccan public health workers. 120
NVivo V.10 software 121 was used to manage the data. Milestones in the coding process were discussed during research team meetings.
Step 5: synthesis
When the data from all sites were analysed, we compared the ICAMO configurations with the initial PT and modified it accordingly. We followed the RAMESES II reporting standards in writing the research report and this paper. 87
Ethical considerations
We informed all interviewees before the start of data collection about the study objectives, topics, type of questions and their right to refuse being interviewed and to interrupt the interview at any time. This information was also provided in an information sheet and reiterated before the start of interview when the written consent procedure was explained. The respondents were asked to sign the informed consent form if they agreed to participate in the study. The forms were cosigned by the researcher and a copy was given to research participants.
Patient and public involvement statement
There was no direct patient involvement in this study.
In this section, we first present for each hospital the main leadership and management practices, the perspective of staff, their views on public service motivation and a summary. Then we present a summary of the cross case analysis and the resulting refined programme theory.
EJM Hospital
Main leadership and management practices.
In EJMH, there were two successive leadership periods. Between 2012 and 2015, CEO 1 had a transactional leadership style, relying on administrative procedures, assertion of power and compliance with rules and procedures. He was perceived by his staff as being distant and not responsive to their needs for professional autonomy. Conflicts and tensions with unions and doctors were high. He left in 2015.
CEO 1 was too strict in the application of the new hospital procedures. We could not discuss the rules with him. The hospital cannot be managed by strictly following the rules. For instance, in compliance with the new procedures, CEO 1 decided to implement night shifts for administrative staff and stopped the night shifts of nursing supervisors. The administrators did not accept to carry out this task because the new procedures did not mention who should do this and how this ‘overtime’ job would be reimbursed. (EJMH 3 administrator)
In mid-2015, CEO 1 was replaced by CEO 2. He was upto then the chief medical officer of the hospital and had quite some management experience. For instance, he was the director of EJMH between 2002 and 2006. In 2016, EJMH won the first price at the quality contest. CEO 2 had an explicit vision on leadership:
I had the chance to manage the hospital in 2002. This allowed me to really know the personal and vice versa. Now, we work as a team in that sense that staff are involved in decision making. This is very important. In a real world setting, participative decision making is very important, because you avoid many problems. When you involve them, you avoid resistance. If staff is involved from the beginning, they will adopt the solution and will not feel that it was imposed on them. This will be totally different if the solution was imposed on the staff. (…) When you involve staff in decision making, you build trust relationships. Trust relationships are very important in our context, where the hospital director has little power over his staff. [….] When we explain to staff well defined objectives. They know which organisational objectives to pursue. Achieving these goals at the operational level bring legitimacy to the hospital direction. It is important that health workers know that you are thriving to achieve these objectives. This is what I call credibility. (EJMH 7, CEO 2)
The perspective of staff
Leadership style.
Our analysis shows that the staff found that the transactional leadership style of CEO 1 was incongruent with their professional values and their need for autonomy. This contributed to mistrust in the management team, low organisational commitment and a high level of tension with unions.
CEO 1, with whom I worked, was authoritative. This was not congruent with my values. I value participative decision making. I try to share with others, I need to be treated the same way by my superior. CEO 1 was just commanding: ‘Do this, give this to this person’. I would have accepted and engaged with him if he would have involved me in participative decision making with other members of the hospital committee, if he would have used polite inquiries, like “Would it be possible to do this?, rather than giving orders without listening to team members or involving them in decision making. (EJMH 25, pharmacist)
The participative decision-making style of CEO 2 and his consideration for individuals restored trust in the management team and reduced the tensions with the unions.
Now everything works smoothly. He does things that are right. He reacts to wrong doings. He is sympathetic with all staff. CEO 2 has a long experience. He knows everyone, he knows their personal characters, motivation and personal needs…. He is very successful in doing that! He knows how to reduce tensions between his close collaborators. He takes decisions smoothly. As a physician, he is able to reduce tensions between medical union representatives and internal coalitions within the medical departments. His door is open to everyone. He listens to staff. He does not rush decisions. He maintains a low level of tension within the hospital. He does not complicate things. The former CEO took rapid decisions and was facing much resistance […]. CEO 2 involves his close collaborators and chiefs of departments in decision making. This way, they adhere to his decisions. He listened to them. He has a participative leadership. (EJMH 25, pharmacist)
Public service motivation
Frontline providers said that compassion and self-sacrifice are important components of their public service motivation.
While recording electrocardiographs on patients, I was constantly communicating with them. Sometimes, women shared with me their feelings, their worries about their siblings, their fear of death, their personal life and stories about their deceased or ill husbands. They were often crying. I feel their sufferings as if I were living with them. (EJMH 17, nurse)
We found that the intrinsic motivation of health providers is sustained by their feelings of competence and their ability to adequately apply their professional skills and competencies.
I love my job. I chose deliberately to work at the emergency unit. I love working at the emergency unit. I am totally engaged. Handling serious medical emergencies is a motivation in itself. (EJMH 38, doctor)
Participative decision-making was perceived by staff as congruent with their professional identity and their public service values. It enhanced their self-esteem and satisfied their needs for autonomy and relatedness and increased their public service motivation. It also increased their perceived autonomy support.
Leaders needs to be fair, listen to our needs and resolve our organizational issues. Most importantly, they need to understand my professional needs, take into consideration my suggestions and contributions to work. This make me feel satisfied. In contrast, with the former leader, I was not feeling secured. He was exerting excessive control. I suffered the martyr!. I was constantly under constant threats. I even sent an administrative correspondence to the ministry of health against the injust treatment. I was just trying to do my job correctly!. (EJMH 17, nurse)
Our analysis showed that the transactional leadership of CEO 1 did not address the basic psychological needs of the staff and specifically the need for autonomy. This not only contributed to low organisational commitment and reduced public service motivation but also to tensions with the unions.
In contrast, CEO 2 had a transformational leadership style: he effectively understood how people are motivated, listened to them and clearly communicated his vision and objectives to the health workers. He showed genuine concern for the needs of his staff, effectively resolving problems through a constructive dialogue with informal leaders and union representatives. He also involved his close collaborators and heads of department in decision-making.
CEO 2 also stimulated the emergence of distributed leadership to lower levels of the organisation, which increased trust between the staff and the CEO, and reduced resistance to change. This was considered by mid-level managers as crucial in maintaining the ‘public service motivation’ of staff, in particular given the perceived limited decision spaces they have over their personal work. We saw that not only senior managers but also mid-level managers engaged in distributing leadership. For the latter, participating in decision-making increased their perceived leader support and satisfaction of their autonomy needs. This has enhanced their autonomous motivation (intrinsic and public service motivation).
RKM Hospital
This hospital has known two leadership periods since 2010. From 2010 to 2012, CEO 1 displayed transactional leadership: he assiduously monitored staff attendance, planned their shifts and dealt with his staff through administrative correspondence. He was confronted with staff resistance.
Because of shortage of intensive care anaesthetists, nurse anaesthetists often take over their tasks, like sedating patients in the operating theatre without medical supervision. When they were confronted with excessive control by the director, they stopped carrying out this ‘medical’ task. This has negatively impacted the continuity of surgical activities. In this case, nurses used their professional expertise as a source for discretionary power (eg, ability to intubate and sedate patients in the operating theatre).
(CEO 1) was suspicious and was strictly applying the regulations to correct the staff absenteeism. When the cat’s away, the mice will play. There were many conflicts, especially with nurse anesthesists who did not comply with the control of attendance. As a result, they stopped sedating patients and argued that they are not allowed to sedate patients without an intensive medical care anaesthetist. (RKMH8, close collaborator)
CEO 2 managed the hospital between 2012 and 2018. He favoured a distant laissez-faire leadership approach and was often absent. He would then be replaced by the chief nursing officer who adopted the same leadership style. The latter seemed overwhelmed by day-to-day operational management responsibilities. During our field work, we noted that the management of the hospital was poor. No organisational action plans were available, and there were no meetings. Strikingly, our FGD with nurses was the only meeting they attended in 3 years. We observed high level of absenteeism among hospital staff.
Our analysis shows that the close collaborators, administrators and technical staff appreciated the leadership of CEO 1 because he reduced role ambiguity and job pressure. However, nurses and doctors were unhappy with his overcontrolling behaviour and engaged in resistance. Also CEO 2 was appreciated by his close collaborators, now because of his gentle wording and good interpersonal management. However, doctors and nurses perceived his laissez-faire leadership as non-responsive to their needs in terms of resources and working conditions. This had led to reduce their public service motivation by reducing their willingness to improve service delivery and to work for the common good. Some have expressed that laissez-faire leadership has catalysed their intention to quit the public sector for good.
Nowadays the strength and pace of my motivation to improve the service quality has decreased. This is essentially due to the lack of responsiveness of the hierarchy to my needs. There is no response. Even though we are engaged to improve our working conditions and the panel of services, the lack of feed back from the management teams has stopped our willingness to improve health service delivery. I found myself complaining alone. This has reduced my attraction to improve public service. This has negatively impacted my psychological well being. In all cases, I get my salary at the end of the month, however, from my personal point of view, I could not contend my self to work without thriving to improve the quality of public service at the pediatric unit. My husband is telling me that improving service delivery in the public sector is not my mission and that I am not a sort of social reformer!!. I am always told that these poor working conditions are common in the public sector and I need to stop trying to work for the common good. My motivation has decreased for while now. But I hope later to try again with the new chief provincial hospital that has recently been appointed. Maybe, he will be more responsive to our needs than the former. If in the coming three years this does not change, I will quit the public sector and start my own private practice. (RKMH 16 paediatrician)
Respondents complained management engaging in clientelism and nepotism, which they found to conflict with their public service values.
The chief of the admission office is carrying out tasks that are not his. He manages the personnel! Staff who come from the town of CEO2 are privileged compared with others. Decisions are guided by his close interpersonal relationship with them. (RKMH 11, nurse) For instance, when I take necessary administrative measures to correct staff absenteeism, the provincial district officer takes no actions to sanction these deviant behaviours. My authority is weakened. Either you accept staff’s deviant behaviours and thus participate in this “crime”, or you are intransigent and staff will build an alliance against you and you will be demonised. As you may know, unions and political parties are corrupt, they seek only the interest of their members and not the general interest. (RKMH 15, administrator)
Staff perceived that they were unable to treat adequately patients because of lack of material and resources (eg, laboratory tests, mobile radiology) and the inadequate organisational support to their supply needs. They did not feel self-efficacious. Some felt that they were doing more harm than good for patients. This reduced their PSM and negatively impacted their psychological well-being.
We suffer because we transfer patients for simple technical procedures that we could have handled locally. (RKMH 10, nurse) We often ask relatives to help us carry patients with a fractured femur to the fixed X Ray table. By doing this, we may worsen the fracture. I feel sorry when I had to ask sick patients to go themselves to the fixed X-Ray table. No organisational support is given, despite our relentless asking the administration to provide us with a mobile X Ray system. (RKMH 14, radiology technician)
Poor management and bad working conditions led to low levels of perceived organisational support among nurses. Staff felt inadequately supported by their supervisors and were left to face problems in the execution of their daily tasks. This created a stressful job pressure they were unable to deal with.
During the transfer (of a patient to the referral hospital), we do not focus on what care to give to the patient, but we are stressed by the poor conditions of the ambulance. It is not an ambulance, it is a wreck! (RKMH 12, nurse anaesthesiologist)
Reluctance of the managers to start up legal procedures against patients or families who assaulted nurses or doctors further reduced the latter’s trust in the management.
Many times, staff were assaulted. The management just forgave the assaulter, because the CEO knows him. Leaders should support staff, … support them in a sense that if someone of us is assaulted one day, I mean a nurse staff in his shift or a doctor, staff should be protected. This assault should not be considered as an assault on an individual person, it is an assault on all of us, on all health care providers cadres in general. (RKMH 24, nurse, ED)
In this hospital, we found that front-line providers value the importance of adequately serving patients and improving health outcomes. They derive satisfaction from relieving suffering and saving lives, or at least preventing them from developing complications. Health workers mentioned that compassion, self-sacrifice, serving the underprivileged and caring for the poor are crucial drivers of their public service motivation.
We often sacrifice our own time for the sake of patients and for the sake of God to avoid unnecessary delays and prevent parturients from getting complications, for exemple, severe neurological and cardiac complications of post partum haemorrhage. We even help patient’s families to pay for ambulance fees in order to avoid delays. (RKMH 14, midwife) Here, I work a lot with vulnerable citizens. It is a reward in itself to serve poor patients. It is my source of motivation. (RKMH 3, doctor)
We noted that the laissez-faire and transactional leadership had a negative effect on staff with high levels of public service motivation. It led to psychological distress, low organisational commitment and self-interested behaviour. This was compounded by the perceived organisational politics (see clientelism and nepotism).
Our analysis showed that the laissez-faire and transactional leadership in this hospital did not respond to the basic psychological needs of health workers. This led to reduced public service motivation with negative consequences on their psychological well-being because of the lack of opportunities of experiencing valued patient outcomes (eg, saving lives).
The leadership styles also contributed to low perceived organisational support, which in a context of perceived organisational politics, in turn lowered organisational commitment, and increased self-interested behaviour and mistrust between administration and staff.
SMBA Hospital
In SMBA Hospital, one of the low-performing hospitals, there were three leadership periods. CEO 1 (2007–2010) displayed strong transactional leadership, emphasising conformity with rules and procedures and insisting on top-down hierarchical management. He carried out many performance audits and clinical supervisions, and organised training to staff. He showed high moral standards and was both respected and feared by staff. He was replaced in 2010 by CEO 2, who retired in 2013. He had some experience in management, displayed transactional leadership and stressed the conformity with rules similar to his predecessor. In 2014, CEO 2 was replaced by CEO 3, who adopted a laissez-faire leadership. The hierarchical line was no longer respected. He managed the hospital poorly: no organisational action plans were available, and he did not carry any audit nor supervision. No inter-unit meetings were held and the departmentalisation process was halted. During our field work, we observed a strike of the clerical officers in charge of hospital admission and of the private company in charge of security in reaction to bad working conditions and perceived low responsiveness of management to their needs.
CEO 1 and 2 were highly appreciated by the administrators and their close collaborators. The health professionals (nurses and doctors) pointed to reduced perceived organisational support and to lack of participative decision-making. Under the leadership of CEO 3, staff felt less supported by their supervisors. They said they were left to deal with problems alone. Lack of clarity of goals led health workers to perceive role ambiguity and job pressure.
Poor management and low responsiveness of leaders to staff needs in terms of improving working conditions decreased their public service motivation.
Leaders do not play a role in our motivation. […]. We came to work despite constraints and poor working conditions. If we were only motivated by working conditions, we wouldn’t come to work. The management team was even unable to timely replace a broken window of our reception desk counter! (SMBA 29, reception desk officer)
Our respondents also mentioned the clientelism and nepotism of CEO 3, who privileged some staff and patients over others. This led to perceived organisational politics and mistrust, and contributed to low organisational commitment, demotivation and crowding out of public service motivation.
In this hospital, there are some external actors who pretend to do social work, and pretend to act as benefactors. These external actors, often members of associations, intervene illegimitely in hospital activities. They are like parasites. They definitely impact on our productivity. They are like stockbrokers. They do not care about citizens. They frequently mediate between citizens and services providers. The CEO responds quickly to patients needs when these actors are involved. This what I call clientelism. This is not fair! All citizens are equal. (SMBA 21, support staff, reception desk)
Physicians and nurses perceived compassion with patients’ conditions and self-sacrifice as major components of their public service motivation.
Patients are important for me because I got sick myself. So, I sense what the patients are feeling. My family members, my daughter and my grandmother got sick. I feel the pain patients are suffering from. I can feel their suffering. (SMBA 35, nurse)
Public service motivation is also driven by religious cultural beliefs including elements of fear of God and divine rewards.
We work because of our sense of humanity, our own consciousness and our fear of God. One day, we will be asked about the quality of work we have done in the past. We feel sorry for patients. (SMBA 29, reception desk officer)
Staff said they were suffering from psychological distress due to poor working conditions, and experienced feelings of guilt because of their inability to perform their job adequately and to ease their patients’ suffering. Lack of opportunities to experience positive patients outcomes reduced their public service motivation.
When you do not have necessary material you are in trouble! It is not only a constraint but a source of suffering. Instead of relieving patients’ distress, it is us who get stressed. (SMBA 45, doctor) Here, ressources are limited compared to the teaching hospital where we were trained. Real world practices are really different. When we first were assigned to this hospital we could not change things around. This is really depressing. We have the ability to provide specialised care but we do not have the necessary ressources to do it! (SMBA 42, doctor)
This impacted negatively on their perceived organisational support. This led to crowding out of their public service motivation and lowered their organisational commitment and their well-being.
It is really depressing. I do not want to work anymore because I do not have the necessary ressources.[…] I often cry when I watch newborns suffering from intramuscular injections because nurses are not skilled to administrater intraveineus infusions to newborns and often use instead intramuscular injection for 10 days. I am not only frustrated, I hate entering neonatology service!!!. I only grudgingly go see my patients whereas in the past I loved providing neonatology care. I cannot stand seeing newborn almost dying of hypoglycaemia 0.3 g/L because they are not adequately fed. This is due to the acute shortage of nurses (one nurse per shift) who are unable to reconciliate between administering antibiotics and treating infections and baby feeding. I am not anymore motivated to cure newborns ‘infections but I am terribly stressed avoiding newborns to die from hypoglycaemia. If babies are left alone with the feeding bottles they may die by suffocation. How can we come motivated to work in the next morning? of course not!!! (SMBA 42, paediatrician)
Shortage of material reduced their ability to properly care for patients, which reduced their PSM and contributed to a reduced sense of competency, self-efficacy and autonomy.
During my pediatric residency, I practiced neonatology and neonatal reanimation for two years, I developped many skills that I am not using now because I do not have the necessary equipments. I have only few neonatal rescuscitation tables and two sources of oxygen for 21 patients. I do not have a respirator. During my training I learned to intubate and manage cardiorespiratory distress. Now, in neonatology service instead of using unavailable syringe pumps,we manage pediatric diabetes by intraveinous perfusion. I never been thaught to do this!!. (SMBA 42, paediatrician) I am very proud to serve my population, however I am truly unsatisfied. We have strong faith and we work eagerly to serve people. But our faith is not sufficiant. We need more ressources. For exemple, I am often called for patients with cranial trauma. We do what is possible depending on available ressources. Cerebral trauma patients need an emergency cerebral CT-scan and the golden hour must be respected. When they arrive at the hospital, often with a delay, the CT Scan is unavailable. It is often out of order. What could we do? In this case, We help teams transfer the patient to the nearby hospital in Marrakech. We often collect money to pay ambulance fuel and to avoid extradelays. I feel that my contribution to patient health is useless, despite being present for about 5 or 6 six hours at night. I feel that our contribution is hampered by organisational problems that are beyond our control. (SMBA 43, intensive care anaesthetist)
In this hospital, we found that leaders (like CEO 1) who are perceived as showing a high sense of moral and ethical standards, and who stimulate the awareness of staff of public service values and their contribution to society, were positively considered by some cadres. For the administrative staff, the transactional leadership displayed by CEO 1 led to higher clarity of goals, reduced job pressure and increased extrinsic motivation. However, it was negatively perceived by frontline workers because they felt it did not respond to their needs for autonomy.
Laissez-faire leadership crowded out public service motivation by reducing frontline healthworkers’ opportunities to help. Such management did not respond to the basic psychological needs of staff and led to low organisational commitment.
In table 3 , we present a summary of the perspectives of staff on the leadership and management practices. We present in the first column the key summary data derived from the initial exploratory case study (NHMH Hospital) and detailed in Belrhiti et al. 88
The perspectives of staff on the leadership and management practices
Cross case analysis and refined causal configurations
Comparing the initial PT with the results of the analysis of the data from the hospitals EJMH, RKMH and SMBA allowed us to refine it ( table 4 ). We used the ICAMO configuration to structure the analysis. 118 We confirmed or refuted the four causal configurations presented above.
Testing the initial configurations in the study sites
ICAMO configuration 1: Laissez-faire leadership and PSM
This configuration was confirmed in the RKMH (CEO 1) and SMBA (CEO 3) hospitals (see table 4 and figure 3 ).

Laissez-faire leadership and PSM (ICAMO 1).
Laissez-faire leadership [I] decreases intrinsic motivation and public service motivation [O] of health providers [A] by being less responsive to the basic psychological needs of autonomy, competence and relatedness [M] and by reducing perceived organisational support [M] in situations of reduced opportunities to experience positive patient outcomes [C].
Laisser-faire leadership [I] contributes to mistrust between administration and staff, resistance to change and tensions with unions [O] by inducing perceived job pressure and role ambiguity [M] for health providers [A].
Laissez-faire leadership [I] reduces public service motivation [O] in a context of perceived organisational politics (clientelism and nepotism) [C] by being incongruent with individual public service values [M] of all cadres [A].
ICAMO configuration 2: transactional leadership and PSM
This configuration is confirmed by empirical data from the three hospitals (EJMH (CEO 1), RKMH (CEO 1), SMBA (CEO 1 and 2)). As a result, we retain ICAMO 2 as follows (see figure 4 ):

Transactional leadership-PSM (ICAMO 2).
If transactional leadership ensures adequate support and working conditions of administrative staff [I] or if enforces a clear hierarchical line [I], it can reduce job pressure [M] and reduce role conflict [M] and thus increase the extrinsic motivation of administrative staff [O] and the level of organisational commitment [O]. If transactional leaders [I] are felt by health professionals [A] to be distant, this can reduce perceived autonomy support and reduce the satisfaction of the need for mutual respect (relatedness) [M], leading in turn to reduced motivation [O] and low organisational commitment [O].
ICAMO configuration 3: transformational leadership and PSM
Configuration 3 is confirmed only in EJMH Hospital (CEO 2) ( figure 5 , table 4 ).

Transformational leadership and PSM (ICAMO 3).
Transformational leadership understood as inspiring staff (walking the talk), infusing jobs with public service values and showing individual consideration to staff [I] increases public service motivation [O] by responding to basic psychological needs of autonomy and relatedness [M] of all staff [A] and contributes to higher organisational commitment and expressed mutual trust between staff with administration [O].
ICAMO configuration 4: distributed leadership and PSM
Distributed leadership was observed only in the high performing hospitals EJMH and NHMH (see figure 6 ).

Distributed leadership and PSM (ICAMO4).
Distributed leadership in the sense of creating a supportive and open climate and good relations between staff [I] increased staff public service motivation [O] and organisational commitment [O] and led to extra role behaviours by satisfying staff basic psychological needs [M] and increasing trust in management teams [M]
As described in tables 3 and 4 , we noticed that only CEO 2 in NHMH and CEO 2 in EJMH displayed complex leadership understood as the balancing between transactional, transformational and distributed leadership that fits best the diversity of professional profiles, the nature of the tasks and the organisational culture. Transactional leadership fits the administrators who value role clarity and reduced job ambiguity, whereas transformational and distributed leadership addresses the basic psychological needs of health providers. The other CEOs either adopted a transactional leadership style or laissez-faire leadership, which was not well received by a majority of staff.
The four ICAMOs presented above allowed us to refine our initial programme theory:
Complex leaders, applying an appropriate mix of transactional, transformational and distributed leadership styles that fit organisational and individual’s characteristics [I] can increase public service motivation, organisational commitment and extra role behaviours [O] by increasing perceived supervisor support and perceived organisational support and satisfying staff basic psychological needs [M], if the organisational culture is conducive and in the absence of perceived organisational politics [C].
In this study, we explored mechanisms and contextual conditions by and in which leadership influences ‘public service motivation’ of health workers.
Our study shows, in line with leadership literature, 122 123 that laissez-faire leadership decreases intrinsic motivation and public service motivation of all cadres by being less responsive to the basic psychological needs of autonomy, competence and relatedness of staff and by reducing perceived organisational support. 1 5 92
Our findings suggest that transactional leadership, when it ensures adequate managerial support and improvement of working conditions, can enhance the extrinsic motivation of staff by reducing role ambiguity and job pressure, and by increasing perceived organisational support. This is supported by other studies. 124–127 However, we also found indications that transactional leadership can crowd out intrinsic motivation and public service motivation of health workers by reducing the satisfaction of their needs for autonomy. This is supported by other studies in LMICs. 40 41 128–130
We found transformational leaders who clearly communicate their vision and walk the talk, infuse jobs with public services meaning, and show individual consideration can enhance PSM by responding to their need for relatedness. This is supported by recent studies. 29 37 56 75 78 131–133 Transactional leadership can lead to higher organisational commitment and extra role behaviours. 134 135
Distributed leadership facilitated teamwork, information flows and team cohesion. It nurtured feelings of connectedness, enhancing the perception of autonomy support and perceived organisational support. This led to creative problem solving, collective learning and better performance at the quality assurance contest, in ways similar to other study findings. 11–15 136
Our study supports the hypothesis that the effect of leadership on PSM depends on the degree of responsiveness to basic psychological needs (autonomy, competency and relatedness). This points to the relevance of self-determination theory 92 106 as a middle range theory that may frame how individual psychological mechanisms underlie the effects of leadership on staff motivation (extrinsic motivation, intrinsic motivation and PSM). It also supports the hypothesis that the effect of leadership on PSM is conditioned by the existence of a conducive organisational culture (a clan culture and absence of perceived organisational politics). This is explained by value congruence, understood as the degree of congruence between individual and organisational values, which represents a major mechanism in the integration of public service values in individual behaviours. 70 75 137 138
In summary, in healthcare organisations, leaders able to adapt their leadership practices to the nature of individuals and organisational characteristics (complex leaders) are likely to be more effective. They foster networking and connections between staff by distributing leadership responsibilities and reinforcing the role of middle managers, infusing jobs with meaning and creating constructive dialogues with professional health workers. 12 61 62 64 139 140
Study contributions, validity and limitations
This study contributed to fill the gap in leadership studies in general 83 141 142 and in healthcare specifically 62 143 by unravelling the underlying mechanisms of leadership effects on health workers’ motivation. It contributes to the study of leadership in North African Muslim countries, a neglected field of research. 144
This study contributes to the case that RE can contribute to building a better understanding of complex phenomena in health systems. 85 RE proved an appropriate approach to unravel the relationship between leadership and PSM, and thus responded to calls of PSM scholars for robust research methodologies. 33 35 37 76 77
The RE proved to be a suitable approach for capturing the multilevel dynamic nature that evolved over time and across contexts. RE facilitated the unveiling of causal mechanisms (value congruence and satisfaction of basic psychological needs) and the contingent effect of contextual factors (organisational culture, climate and perceived organisational politics) and the individual reasoning of different social actors (eg, perceived supervisor and organisational support). 85 145 146
By using ICAMO configurational analysis, we were able to provide evidence on the contextual nature and social construction of leadership. Adopting a situational approach on leadership help overcome the inconsistency of findings when studying leadership effectiveness in organisations. 147–149
In addition, the qualitative multiple embedded case study design proved appropriate in providing qualitative design rich, dynamic, contextual data with a focus on mechanisms rather than variables. 150 Qualitative approaches are complex sensitive and allow for more research flexibility in unveiling the mechanisms and conditions underlying complex social phenomena in general and more specifically leadership effectiveness in health. 98 150–153
The validity of our study findings is derived from theoretical guidance in study design, sampling and analysis, and cross-validation 154–156 and theoretical replication across cases. 119 Theoretical replication allows for a retroductive process of knowledge creation 119 by constantly shuttling from theory to empirical data and by continuously refining our programme theories across negative and positive cases.
There are limitations to our study. The causal configurations developed here are the most plausible explanation for the outcomes observed in our study, but may likely not be the unique explanation. Further empirical testing in a larger set of cases would enable to further refine the PTs. A second limitation is that we did not quantitatively measure public service motivation, organisational commitment, perceived organisational support and other variables. The time and resource limits of the PhD study, of which the study presented here is part, precluded testing and validating existing scales for these constructs.
Implications for practice
In Morocco, similar to other LMICs, 56 the hierarchical culture within the Ministry of Health favours transactional leadership styles 49 157 and this may impede the emergence of PSM. 158–160 We raise some concerns in relation to the actual health reforms carried out in Morocco, which are inspired by new public management (eg, performance-based management, contracting out and public–private partnerships) and which may have negative consequences on health workers’ performance by facilitating the practice of transactional leadership, focusing on extrinsic rewards (and sanctions) and crowding out the expression of PSM and self-altruistic behaviours of frontline health workers. Policy makers should stimulate the development of complex leadership competencies (eg, fostering network building, generative sense making, see also Belrhiti et al 62 in their capacity building programme.
In the context of healthcare organisations, the motivation of health workers relies on individual, organisational and contextual antecedents. The effectiveness of leaders depends on the degree of responsiveness to the basic psychological needs of health workers and on value congruence between organisational and individual values. Leaders should learn how to adapt their leadership practices to the organisational characteristics (nature of task, mission valence) and to type of motivation of health workers (extrinsic vs intrinsic and PSM). Further research is needed to explore the role of value congruence and to understand how the social institutions (ie, religion, family education, professionalism) may shape the expression of public service motivation of health workers in LMICs.
Supplementary Material
Twitter: @drbelrhiti
Contributors: All the four authors (ZB, BM, WVD, AB) contributed to the original design and analysis and writing of the manuscript. ZB carried out the data collection. BM cross checked the transcripts. Initial coding was done by ZB and discussed between the research team members (BM, WVD, AB). ZB edited the final draft. All authors read and approved the final manuscript.
Funding: This work was funded through a PhD framework agreement between the Belgian Directorate-General for Development Cooperation and the Institute of Tropical Medicine, Antwerp. The sponsors had no role in the study or in the writing of the paper.
Competing interests: None declared.
Patient consent for publication: Not required.
Ethics approval: The research protocol was approved by the Moroccan Institutional Review Board (No. 90/16) of the Faculty of Medicine of Pharmacy, Rabat and the Institutional Review Board of the Institute of Tropical Medicine, Antwerp (No. 1204/17). All participants have been informed prior to the conduct of the research and written consent forms were signed by the respondents and countersigned by the researcher. A signed copy was given to each respondents.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data availability statement: Data sharing not applicable as no datasets generated and/or analysed for this study.

Top 40 Most Popular Case Studies of 2021
Two cases about Hertz claimed top spots in 2021's Top 40 Most Popular Case Studies
Two cases on the uses of debt and equity at Hertz claimed top spots in the CRDT’s (Case Research and Development Team) 2021 top 40 review of cases.
Hertz (A) took the top spot. The case details the financial structure of the rental car company through the end of 2019. Hertz (B), which ranked third in CRDT’s list, describes the company’s struggles during the early part of the COVID pandemic and its eventual need to enter Chapter 11 bankruptcy.
The success of the Hertz cases was unprecedented for the top 40 list. Usually, cases take a number of years to gain popularity, but the Hertz cases claimed top spots in their first year of release. Hertz (A) also became the first ‘cooked’ case to top the annual review, as all of the other winners had been web-based ‘raw’ cases.
Besides introducing students to the complicated financing required to maintain an enormous fleet of cars, the Hertz cases also expanded the diversity of case protagonists. Kathyrn Marinello was the CEO of Hertz during this period and the CFO, Jamere Jackson is black.
Sandwiched between the two Hertz cases, Coffee 2016, a perennial best seller, finished second. “Glory, Glory, Man United!” a case about an English football team’s IPO made a surprise move to number four. Cases on search fund boards, the future of malls, Norway’s Sovereign Wealth fund, Prodigy Finance, the Mayo Clinic, and Cadbury rounded out the top ten.
Other year-end data for 2021 showed:
- Online “raw” case usage remained steady as compared to 2020 with over 35K users from 170 countries and all 50 U.S. states interacting with 196 cases.
- Fifty four percent of raw case users came from outside the U.S..
- The Yale School of Management (SOM) case study directory pages received over 160K page views from 177 countries with approximately a third originating in India followed by the U.S. and the Philippines.
- Twenty-six of the cases in the list are raw cases.
- A third of the cases feature a woman protagonist.
- Orders for Yale SOM case studies increased by almost 50% compared to 2020.
- The top 40 cases were supervised by 19 different Yale SOM faculty members, several supervising multiple cases.
CRDT compiled the Top 40 list by combining data from its case store, Google Analytics, and other measures of interest and adoption.
All of this year’s Top 40 cases are available for purchase from the Yale Management Media store .
And the Top 40 cases studies of 2021 are:
1. Hertz Global Holdings (A): Uses of Debt and Equity
2. Coffee 2016
3. Hertz Global Holdings (B): Uses of Debt and Equity 2020
4. Glory, Glory Man United!
5. Search Fund Company Boards: How CEOs Can Build Boards to Help Them Thrive
6. The Future of Malls: Was Decline Inevitable?
7. Strategy for Norway's Pension Fund Global
8. Prodigy Finance
9. Design at Mayo
10. Cadbury
11. City Hospital Emergency Room
13. Volkswagen
14. Marina Bay Sands
15. Shake Shack IPO
16. Mastercard
17. Netflix
18. Ant Financial
19. AXA: Creating the New CR Metrics
20. IBM Corporate Service Corps
21. Business Leadership in South Africa's 1994 Reforms
22. Alternative Meat Industry
23. Children's Premier
24. Khalil Tawil and Umi (A)
25. Palm Oil 2016
26. Teach For All: Designing a Global Network
27. What's Next? Search Fund Entrepreneurs Reflect on Life After Exit
28. Searching for a Search Fund Structure: A Student Takes a Tour of Various Options
30. Project Sammaan
31. Commonfund ESG
32. Polaroid
33. Connecticut Green Bank 2018: After the Raid
34. FieldFresh Foods
35. The Alibaba Group
36. 360 State Street: Real Options
37. Herman Miller
38. AgBiome
39. Nathan Cummings Foundation
40. Toyota 2010
CONCEPTUAL ANALYSIS article
Role of institutions in public management: developing case studies for divergent policy systems provisionally accepted.

- 1 XIM University, India
The final, formatted version of the article will be published soon.
Public policy management has an intractable nature, and the institutional complexity of governance further exacerbates its practice. Transnational learning cutting across countries and policy areas can contribute to this policy knowledge in dealing with multifarious issues in public management. Understanding the institutional mix in public management in various contexts enhances the existing comprehension of how the national pattern of public management works differently in different socio-economic, cultural, and political settings. The present research aims to study the institutional framework in the form of state structure (unitary or federal) and the nature of executive government (majoritarian or consensual) in delineating the influence of institutions on public management processes in divergent policy systems. The paper undertakes four in-depth country case studies and the public management reforms as a response to institutional pressure are examined using the 4M strategy (Pollitt and Bouckaert, 2017)-Maintain (holding on to existing administrative structures and processes), Modernize (keeping service delivery and regulation up to date), Marketize (efficiency and user-responsive public management), and Minimize (reducing state-led regulation). The case studies highlight the differences in the broad direction and energy of implementation that characterize a particular policy style. The results of the study indicate that even though the institutional dimensions are not present in strict polarization, the impact of the institutional mix is evident in the dominant strategies of public management reforms adopted at the national level.
Keywords: political executive, Institutionalism and institutions, Public management, State Structure, Comparative politics
Received: 14 Jul 2023; Accepted: 05 Apr 2024.
Copyright: © 2024 Singh. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY) . The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
* Correspondence: Dr. Vaishali Singh, XIM University, Bhubaneswar, India
People also looked at
- Skip to main content
- Keyboard shortcuts for audio player
Millions of customers' data found on dark web in latest AT&T data breach

Chloe Veltman

An AT&T store in New York. The telecommunications company said Saturday that a data breach has compromised the information tied to 7.6 million current customers. Richard Drew/AP hide caption
An AT&T store in New York. The telecommunications company said Saturday that a data breach has compromised the information tied to 7.6 million current customers.
AT&T announced on Saturday it is investigating a data breach involving the personal information of more than 70 million current and former customers leaked on the dark web.
According to information about the breach on the company's website, 7.6 million current account holders and 65.4 million former account holders have been impacted. An AT&T press release said the breach occurred about two weeks ago, and that the incident has not yet had a "material impact" on its operations.
AT&T said the information included in the compromised data set varies from person to person. It could include social security numbers, full names, email and mailing addresses, phone numbers, and dates of birth, as well as AT&T account numbers and passcodes.
The company has so far not identified the source of the leak, at least publicly.
"Based on our preliminary analysis, the data set appears to be from 2019 or earlier," the company said. "Currently, AT&T does not have evidence of unauthorized access to its systems resulting in theft of the data set."

AT&T says cell service is back after a widespread outage and some disrupted 911 calls
The company said it is "reaching out to all 7.6 million impacted customers and have reset their passcodes," via email or letter, and that it plans to communicate with both current and former account holders with compromised sensitive personal information. It said it plans to offer "complimentary identity theft and credit monitoring services" to those affected by the breach.
External cybersecurity experts have been brought in to help investigate, it added.
NPR reached out to a few AT&T stores. The sales representatives in all cases said they were as yet unaware of the breach.
On its website, the telecommunications company encouraged customers to closely monitor their account activity and credit reports.
"Consumers impacted should prioritize changing passwords, monitor other accounts and consider freezing their credit with the three credit bureaus since social security numbers were exposed," Carmen Balber, executive director of the consumer advocacy group Consumer Watchdog, told NPR.
An industry rife with data leaks
AT&T has experienced multiple data breaches over the years.
In March 2023, for instance, the company notified 9 million wireless customers that their customer information had been accessed in a breach of a third-party marketing vendor.
In August 2021 — in an incident AT&T said is not connected to the latest breach — a hacking group claimed it was selling data relating to more than 70 million AT&T customers. At the time, AT&T disputed the source of the data. It was re-leaked online earlier this month. According to a Mar. 22 TechCrunch article , a new analysis of the leaked dataset points to the AT&T customer data being authentic. "Some AT&T customers have confirmed their leaked customer data is accurate," TechCrunch reported. "But AT&T still hasn't said how its customers' data spilled online."
AT&T is by no means the only U.S. telecommunications provider with a history of compromised customer data. The issue is rife across the industry. A 2023 data breach affected 37 million T-Mobile customers. Just last month, a data leak at Verizon impacted more than 63,000 people, the majority of them Verizon employees.
A 2023 report from cyber intelligence firm Cyble said that U.S. telecommunications companies are a lucrative target for hackers. The study attributed the majority of recent data breaches to third-party vendors. "These third-party breaches can lead to a larger scale supply-chain attacks and a greater number of impacted users and entities globally," the report said.
Government rules adapt
Meanwhile, last December, the Federal Communications Commission (FCC) updated its 16-year-old data breach notification rules to ensure that telecommunications providers adequately safeguard sensitive customer information. According to a press release , the rules aim to "hold phone companies accountable for protecting sensitive customer information, while enabling customers to protect themselves in the event that their data is compromised."
"What makes no sense is leaving our policies stuck in the analog era," said FCC Chairwoman Jessica Rosenworcel in a statement regarding the changes. "Our phones now know so much about where we go and who we are, we need rules on the books that make sure carriers keep our information safe and cybersecure."
- data breach
- Open access
- Published: 03 April 2024
Trends in antidiabetic drug use and expenditure in public hospitals in Northwest China, 2012-21: a case study of Gansu Province
- Wenxuan Cao 1 ,
- Hu Feng 1 ,
- Yaya Yang 1 ,
- Lei Wang 1 ,
- Xuemei Wang 1 ,
- Yongheng Ma 2 ,
- Defang Zhao 2 &
- Xiaobin Hu 1
BMC Health Services Research volume 24 , Article number: 415 ( 2024 ) Cite this article
35 Accesses
Metrics details
Since the twenty-first century, the prevalence of diabetes has risen globally year by year. In Gansu Province, an economically underdeveloped province in northwest China, the cost of drugs for diabetes patients accounted for one-third of their total drug costs. To fundamentally reduce national drug expenditures and the burden of medication on the population, the relevant departments of government have continued to reform and improve drug policies. This study aimed to analyse long-term trends in antidiabetic drug use and expenditure in Gansu Province from 2012 to 2021 and to explore the role of pharmaceutical policy.
Data were obtained from the provincial centralised bidding and purchasing (CBP) platform. Drug use was quantified using the anatomical therapeutic chemistry/defined daily dose (ATC/DDD) method and standardised by DDD per 1000 inhabitants per day (DID), and drug expenditure was expressed in terms of the total amount and defined daily cost (DDC). Linear regression was used to analyse the trends and magnitude of drug use and expenditure.
The overall trend in the use and expenditure of antidiabetic drugs was on the rise, with the use increasing from 1.04 in 2012 to 16.02 DID in 2021 and the expenditure increasing from 48.36 in 2012 to 496.42 million yuan in 2021 (from 7.66 to 76.95 million USD). Some new and expensive drugs changed in the use pattern, and their use and expenditure shares (as the percentage of all antidiabetic drugs) increased from 0 to 11.17% and 11.37%, but insulins and analogues and biguanides remained the most used drug class. The DDC of oral drugs all showed a decreasing trend, but essential medicines (EMs) and medical insurance drugs DDC gradually decreased with increasing use. The price reduction of the bid-winning drugs was over 40%, and the top three drugs were glimepiride 2mg/30, acarbose 50mg/30 and acarbose 100mg/30.
Conclusions
The implementation of pharmaceutical policies has significantly increased drug use and expenditure while reducing drug prices, and the introduction of novel drugs and updated treatment guidelines has led to changes in use patterns.
Peer Review reports
About one in ten of the world's population is diabetes patient, and what's worse is that this percentage is increasing every year. According to the International Diabetes Federation, in 2021, 537 million adults (aged 20–79) worldwide had diabetes, resulting in an estimated total global healthcare expenditure of 966 billion USD [ 1 ]. China had the largest number of diabetes patients in the world. According to statistics, approximately 11.2% of adults aged 18 years and older had diabetes in 2021, with the total number of patients reaching 141 million, and it was expected to reach 174 million by 2045 [ 2 ].
Gansu Province is an economically underdeveloped province in northwestern China, and a study showed that the local diabetes prevalence rate was 7.33% in 2018 [ 3 ]. In the same year, the total healthcare cost of diabetes patients was 1.348 billion yuan (20.37 million USD) [ 4 ], accounting for 2.56% of the total treatment cost in the province and 0.16% of the regional gross domestic product (GDP). Although this percentage was not high, the cost of drugs accounted for about one-third, which was much higher than the average level of 19.7% among the member countries of the Organisation for Economic Co-operation and Development in 2019 [ 5 ].
Appropriate use of antidiabetic drugs is key in the management of diabetes (especially type 2 diabetes), which is important for delaying disease progression, reducing the risk of complications and reducing the disease burden. To fundamentally reduce national drug expenditure and the burden of drug use on the population, relevant Chinese government departments have been reforming and improving their drug policies. The National Essential Medicine System (NEMS) was first established in 2009, provinces and cities across the country have started to implement the "three unified" (policies of unified bidding, distribution, and pricing) and zero-price markup policy to expand the coverage of essential medicines (EMs) [ 6 ]. And all EMs were included in the National Basic Medical Insurance Drug Catalogue (NBMIDC), so their reimbursement rate was higher than that of non-EMs. As Chinese residents' basic medical insurance coverage was upwards of 95% [ 7 ], this policy significantly reduced out-of-pocket payment for residents.
Since the beginning of the three-year new medical reform (2009–11), Gansu has involved government-run medical and health institutions in the scope of the national EMs management and has achieved zero mark-up drugs——No mark-ups or other surcharges are allowed in the price of medicines, the actual selling price is close to the cost price. By the end of 2012, the coverage rate of the EMs system reached 100%. After the policy came to maturity, it successfully reduced the drug cost share from 34.98% in 2014 to 26.91% in 2018 within four years [ 8 ]. At the same time actively implementing the national centralised drug procurement policy, until 2021, Gansu Province has carried out the national organization of five batches of 218 drugs centralized procurement work, which contained a total of 14 varieties (based on Anatomical Therapeutic Chemical (ATC) -5), 23 strains (based on formulations, dosage specifications and manufacturers) of antidiabetic drugs [ 9 , 10 , 11 , 12 , 13 ]. According to incomplete statistics from relevant government departments, the policy has led to an average price reduction of 54.6% for the drugs included and relative cost savings of more than 1.3 billion yuan (20.15 million USD) [ 14 ]. To date, several studies have reported on temporal trends in the use of antidiabetic drugs in other foreign countries, but few studies have focused on changes in the use and expenditure of this class of drugs in less economically developed areas of China and the role of pharmaceutical policies behind the changes [ 15 , 16 ].
This study collected data on antidiabetic drugs in Gansu Province from 2012 to 2021, aiming (1) to explore the long-term trends and use patterns of antidiabetic drug use and expenditure in Northwest China, (2) to reveal the impact of the implementation of pharmaceutical policy on drug use and DDC.
Study setting
Gansu Province is in northwest China, with a narrow and curving topography, and is an economically underdeveloped province. The province's GDP was 102.43 billion yuan (15.88 billion USD) in 2021——the fifth lowest in the country [ 17 ]. With over 70% of the population living in rural, the dispersed nature of the population due to geography and economic level, limited medical resources and inadequate public health education were the main reasons that prevented diabetes patients in the region from effectively managing their disease [ 18 ]. The residents' health insurance coverage was over 97%, and the patient's medical expenses were shared between the national health insurance (coordinated payment) and the patient (individual out-of-pocket payment) within reasonable reimbursement limits [ 19 ].
Data source
The study used data from the centralised bidding and purchasing (CBP) platform managed by the Drug Procurement Division of the Gansu Provincial Public Resources Transaction Center. Its main record information included the drug’s generic name, dosage form, specification, conversion factor, approval number, manufacturer, purchasing unit, purchasing time, purchasing quantity and amount. By 2020, the number of hospitals covered by this database accounted for 93.39% of the total number of public hospitals. This study adopted a retrospective research method, based on the daily drug procurement data of public hospitals in the province from 2012 to 2021, to sort out a total of 2 major categories (based on ATC-3), 10 subcategories (based on ATC-4), 40 varieties (based on ATC-5) and 338 strains (based on formulations, dosage specifications and manufacturers) of antidiabetic drugs, basically covering the main types of diabetes therapeutic drugs. In China, all antidiabetic drugs approved by the healthcare authorities are prescription drugs, and diabetes patients must be prescribed them by clinicians and obtained from hospital pharmacies.
Data management
The ATC system classified drugs into different groups according to the organ or system on which they act and chemical, pharmacological and therapeutic properties. Drugs were classified into ATC groups by its international non-proprietary name. In this paper, all "A10" (drugs used in diabetes) in "A" (alimentary tract and metabolism) were included in the study. Among them, we emphasized the use of a novel antidiabetic drug group, with the following ATC codes: A10BH and A10BD07-13 for dipeptidyl peptidase 4 inhibitors (DPP-4i); A10BJ, A10AE54 and A10AE56 for glucagon-like peptide-1 receptor analogue (GLP-1RAs); A10BK, A10BD15 and A10BD20 for sodium-glucose co-transporter 2 inhibitors (SGLT2i) [ 20 ].The data was analysed using the ATC/defined daily dose (DDD) system developed by the WHO [ 21 ], which calculated the frequency of use of defined daily doses (DDDs) and the defined daily cost (DDC) of each drug based on the DDD, and expressed the standardised dosing intensity in terms of doses per 1000 inhabitants per day (DID). The DDD is the average daily dose used in adults for the primary therapeutic purpose, based mainly on the DDD values of drugs published on the official website; DDDs and DDC were calculated using the following formula, the higher the DDDs, the more frequently such drugs were used and the greater the clinical tendency to choose the drug; the higher the DDC, the greater the financial burden on the patient.
where N i represents the number of packages of drug ( i ).
Data analysis
The number of residents per year was expressed as the average of the population at the end of that year and the previous year in the Gansu Statistical Yearbook (mid-year population) [ 22 ], on the basis of which the number of permanent residents was adjusted using data on the mobile population in Gansu Province [ 23 ] in order to reduce any possible errors in the results that may result from this. Expenditure was adjusted for price inflation at an annual rate of 1.42% (the average annual inflation rate of the Gansu provincial consumer price index from 2012 to 2021) [ 24 ]. Descriptive statistics were used to describe the annual use and expenditure of antidiabetic drugs in Gansu Province, and to calculate the use shares (as the proportion of the total use) and DDC values of each drug type. Linear regression was used to analyse the changes in the use and expenditure of each type of drug during the study period (at least five consecutive years of purchase records), and the regression coefficients ( B value) and significance ( P value) were used to indicate the direction of the trend. Whether the B value is greater than 0 indicates the direction of change (> 0—upward, < 0—downward), and P values < 0.05 were taken to indicate statistical significance. Microsoft Office Excel 2016 and Stata 16.0 were used for data management and analysis, and GraphPad Prism 9 was used for graphing.
Overview of the use of antidiabetic drugs
During the ten-year study period, the overall trend of antidiabetic drug use and expenditure in Gansu Province was increasing ( B = 1.373, 44.229, P < 0.001), use increased from 1.04 in 2012 to 16.02 DID in 2021, and expenditure increased from 48.36 in 2012 to 496.42 million yuan in 2021 (from 7.66 to 76.95 million USD), with the largest increase in 2013 and the largest decrease in 2018.
There were large differences in the composition of use by drug class. Insulins and analogues were the most used, but their proportion of use decreased by almost 20% over the decade ( B = -0.048, P < 0.001). In contrast, the proportion of use of oral antidiabetic drugs remained mostly stable or increased. For example, the proportion of use of biguanides increased by about 10% ( B = 0.017, P = 0.002), the proportion of use of sulfonylureas remained stable at about 20%, followed by α-glucosidase inhibitors, its proportion of use increased rapidly to one-fifth of the total ( B = 0.272, P = 0.001) (Fig. 1 ).

Trends in the use and proportion of antidiabetic drugs. A trends in the use of antidiabetic drugs; B trends in the proportion of antidiabetic drugs. GLP-1RAs, glucagon-like peptide-1 receptor analogues; SGLT2, sodium-glucose co-transporter 2; DDD, defined daily dose
Among the different hospital levels, the use was comparable between tertiary and secondary hospitals (44.19% vs 42.18%) and lowest in primary hospitals (13.63%). Drug use increased in all hospital levels during the study period but with a gradual decrease in the proportion of drugs used in tertiary hospitals ( B = -0.010, P = 0.029) and an increasing trend in the proportion of drugs used in secondary ( B = 0.009, P = 0.042) (Fig. 2 ).

Trends in the use and proportion of antidiabetic drugs in different hospital levels. A trends in the use of antidiabetic drugs in different hospital levels; B trends in the proportion of antidiabetic drugs in different hospital levels. PHCs, primary health care centres; DDD, defined daily dose
Trends in the use of novel antidiabetic drugs
The total use ( B = 0.420, P = 0.034) and expenditure ( B = 13.529, P = 0.008) of novel antidiabetic drugs have continued to increase since 2017, and their shares reached 11.17% and 11.37% of the total by 2021 respectively. The most widely used class of novel antidiabetic drugs was SGLT2i, accounting for 56.67% of the total use in this group, followed by DPP-4i and GLP-1RAs with 30.83% and 10.68% respectively.
Trends in DDC for different classes of antidiabetic drugs
For the different classes of antidiabetic drugs, the top three drug classes in terms of DDC were GLP-1RAs (¥12.81), combinations of oral blood glucose lowering drugs (¥12.66), insulins and analogues (¥11.79), and the bottom three were sulfonylureas (¥1.17), biguanides (¥1.80) and SGLT2i (¥2.58), with the highest class having an average annual DDC of about 11 times that of the lowest class.
The mean DDC of all antidiabetic drugs showed a decreasing trend over the study period ( B = -0.0250, P = 0.044), with an average decrease of 4 percentage points per year, and this trend was evident after 2017. The DDC of insulins and analogues increased from year to year ( B = 0.458, P < 0.001), whereas the DDC of the remaining oral antidiabetic drugs showed a decreasing trend, with significant decreases for SGLT2i (-26.64%), α-glucosidase inhibitors (-13.74%) and other blood glucose lowering drugs (-7.23%) (Table 1 ).
The impact of pharmaceutical policy on drug use and expenditure
Based on the ems perspective.
The overall trend in the share of use and expenditure of EMs was slowly increasing during the study period, and the relative ratio with fixed base for both was almost the same (18.88% vs. 18.24%). In terms of DDC for both types of drugs, both EMs and non-EMs showed a decreasing trend, but the decrease for EMs was significantly higher than non-EMs (-35.93% vs. -8.84%) (Fig. 3 A).

Trends in the use and DDC of EMs and medical insurance drugs. A trends in the use and DDC of EMs and non-EMs; B trends in the use and DDC of medical insurance and non-medical insurance drugs. DDC, defined daily cost; EMs, essential medicines
Based on the medical insurance classification perspective
Both the use and expenditure shares of medical insurance drugs tended to increase during the study period ( B = 0.022, 0.030, P = 0.024, 0.009), with a significantly higher relative ratio with fixed base in expenditure than in use (28.69% vs. 14.76%). In terms of DDC for both types of drugs, both medical insurance and non-medical insurance drugs showed a decreasing trend, but the decrease for non-medical insurance drugs was significantly higher than for medical insurance (-61.80% vs. -27.77%) (Fig. 3 B).
Based on the perspective of the centralised procurement
The impact of the centralised procurement policy on the use and expenditure of the bid-winning drugs was found to be accompanied by a short-term response to the implementation of each policy, with a significant increase in use and a significant decrease in expenditure, ultimately manifesting as a "precipitous" decrease in the DDC of the bid-winning drugs. Among them, the second batch of bid-winning drugs had the largest increase in use (189.91%) and expenditure (-76.32%) after the policy, while the impact on the fourth and fifth batches of bid-winning drugs was relatively small (Fig. 4 ).

Trends in the use and expenditure of bid-winning drugs under the centralised procurement policy. A trends in the use of bid-winning drugs; B trends in the expenditure of bid-winning drugs. DDDs, defined daily doses; DDC, defined daily cost
In terms of DDC, the price reductions for all batches of bid-winning drugs were above 40%, again with the largest price reduction (81.71%) for the second batch of bid-winning drugs. Among the six antidiabetic drugs with records of use before the implementation of the policy, the top three price reductions were for glimepiride 2mg/30, acarbose 50mg/30 and acarbose 100mg/30, with price reductions of 6.43% (¥1.31), 8.45% (¥11.81) and 9.55% (¥8.81) in that order (Table 2 ).
The global prevalence and incidence of diabetes have risen dramatically since the beginning of the twenty-first century [ 25 ]. As diabetes and its early complications were heavily dependent on medication, this changing disease prevalence trend inevitably led to a continued increase in the use of related drugs. In addition, as the level of drug development has improved, new and more expensive antidiabetic drugs with better efficacy and fewer side effects have been included in the recommended treatment guidelines [ 26 ] and have been introduced to the market, which have also contributed to a significant increase in drug expenditure. Ultimately, the three main reasons were the ageing of the world's population, the decline in mortality from diseases triggered by improvements in health care, and the decreasing risk factors for disease [ 27 ].
Notwithstanding the trends above, the level of use and expenditure on antidiabetic drugs in Gansu Province was much lower than in some economically developed countries and regions worldwide, and was even comparable to that of Denmark at the end of the twentieth century [ 15 , 20 , 28 , 29 ]. This is partly because the prevalence rate in Gansu Province was lower than in these countries, and the knowledge and treatment of diabetes are lower, another partly because the consumption of medicines in retail pharmacies was not yet included in our study, resulting in an underestimation of the overall use [ 30 ]. To reduce the burden of drugs on the grass-roots population, the relevant departments of the Gansu Provincial Government have in recent years continued to update the medical insurance policy for the two diseases, including the expansion of the scope of outpatient medication services, the upward adjustment of the overall reimbursement rate, the implementation of long-term prescription management and the implementation of instant settlement at the place of medical treatment, among other things [ 31 ]. In the future, publicity efforts should also be further stepped up, and with the help of new technologies such as artificial intelligence, big data and cloud computing, personalised health management, proactive follow-up and lifestyle intervention should be carried out for the key groups of people with chronic diseases, to reduce the waste of medical resources due to the unregulated management and treatment of chronic diseases.
The composition of the use of different classes of antidiabetic drugs in Gansu Province varied greatly. Among the oral antidiabetic drugs, biguanides overtook sulfonylureas to jump to first place, and α-glucosidase inhibitors caught up to become the third most used oral antidiabetic drug. To the present time, as these facts are still true——hypoglycemia is one of the dangerous complications of diabetes. Because sulphonylureas tended to trigger weight gain and hypoglycemia in patients [ 32 ], international guidelines preferred metformin, which did not increase the risk of hypoglycemia. This drug was still the most widely used first-line treatment in most countries because it combined safety and cost-effectiveness [ 33 ]. And for patients with the limited effect of single drug therapy, multiple combinations of metformin and other oral antidiabetic drugs or injectable drugs were used to control blood glucose. The use of α-glucosidase inhibitors was higher in Gansu Province compared to the United States and some European countries. Due to a diet with carbohydrates as a core food and genetic differences, most Chinese had higher postprandial blood glucose levels than Europeans [ 34 ], and α-glucosidase inhibitors were widely used to treat type 2 diabetes in Chinese patients because their mechanism of action was to lower postprandial blood glucose levels by inhibiting the absorption of carbohydrates in the upper small intestine [ 35 ].
As a representative of the novel antidiabetic drug group, dapagliflozin was approved for entry into China in March 2017, becoming the first SGLT2i to be marketed in China, and in the same year sitagliptin, which belonged to DPP4i, was added to the NBMIDC (Class B) [ 36 ], both of which have contributed to the increased use of this drug group. Of course, another reason could be that the use base in the early days was too small. The proportion of novel antidiabetic drugs in Gansu Province has continued to increase over the past five years, with SGLT2i accounting for the highest proportion (about three-fifths), followed by DPP4i, despite being the first novel antidiabetic drug to enter China. Due to the wide disparity in economic and educational levels between urban and rural residents, the rate of early diagnosis and effective treatment of diabetes patients in rural areas of China was low, and patients often waited until they developed serious complications before receiving treatment. Some studies have shown that the incidence of complications in Chinese diabetes patients was higher than in some high-income countries, especially in cardiovascular complications and kidney damage [ 37 ]. SGLT2i had good efficacy in treating these complications of diabetes, and the inclusion of this class of drugs in the NBMIDC has resulted in more significant price reductions, which may be a reasonable explanation for the above phenomenon.
The results of the study showed that diabetes treatment in Gansu Province was still concentrated in secondary and tertiary hospitals, and there was no gradual downward trend toward primary health care. Despite the Chinese government's commitment to managing and treating chronic diseases through the primary health care system over the past few decades, including a significant increase in investment in health care resources and human resources [ 38 ], an unexpectedly large number of residents still tended to bypass nearby primary health care facilities in favour of higher-level facilities for the treatment of minor ailments. The reason for this was that residents living in urban areas choose high-level hospitals because of their proximity, while as mentioned earlier, some rural residents can only choose high-level hospitals because of the severity of their illnesses [ 39 ].
The DDC of different classes of antidiabetic drugs varied considerably, and there is no doubt that insulins and analogues and novel antidiabetic drugs were generally more expensive, which is consistent with other studies [ 40 ]. The price of combinations of oral antihyperglycemic drugs was also high. The combination of metformin and thiazolidinediones was the most used compounded hypoglycemic drug in Gansu Province, followed by and novel antidiabetic drug group, which was the main reason for the high price of this class of drugs. In addition to the limitations of the ATC/DDD evaluation system used in the study for the treatment of combinations of oral blood glucose lowering drugs dosage, which also caused the inflated DDC of this class of drugs to some extent.
The use of antidiabetic drugs in Gansu Province has been shifting towards EMs, while gradually moving towards medically insured drugs, and more high-priced drugs were included in the NBMIDC. This phenomenon has been reported in other studies [ 41 ]. Two key aspects of drug policy were pricing and reimbursement. In China, provincial governments set uniform procurement prices for their regions within the national guideline price range based on tenders to ensure reasonable value for money [ 42 ]. The inclusion of drugs in the NBMIDC meant that pharmaceutical companies could own the majority of the public hospital market, so companies were often willing to "trade volume for price" [ 43 ]. At the same time, high health insurance coverage played a benign role in reducing the financial burden of illness on the population and reducing catastrophic health expenses for families, especially for chronic diseases [ 44 ]. For the phenomenon of rapid decline in the price of non-medical insurance drugs, which does not exclude enterprises in the bidding for the sake of immediate interests, and was made regardless of the cost of "irrational price reduction" behaviour [ 45 ]. This is not a good trend, in the long run will not only lead to the supply of drugs but also not be conducive to the research and development of innovative drugs.
In 2019, the Chinese government launched the first round of national centralised drug procurement to reduce drug prices and save drug costs through economies of scale [ 46 ]. Available studies have shown that the implementation of this policy has significantly reduced the DDC of bid-winning drugs, including some common chronic disease drugs (e.g. antihypertensive drugs) and acute disease drugs (e.g. emergency drugs) [ 47 , 48 ]. As the results show, the DDC of each batch of bid-winning drugs in Gansu Province has experienced a "precipitous" decline, accompanied by a significant increase in dosage, which showed that patients' medication is generally concentrated in the bid-winning drugs. As the number of bid-winning drugs continues to increase in the future, it will be conducive to improving the overall quality of medication for diabetes patients in China and reducing the burden of medication to a greater extent. However, it is worth noting that most of the drugs have only been procured and used since they were selected, reflecting the strong policy guidance on drug selection, which also placed higher demands on the quality of the winning product.
The study has some limitations. Firstly, the data used in the study were procurement data, which may not directly reflect the actual use of antidiabetic drugs. Secondly, the procurement hospitals included in the study were all public healthcare institutions, so the results can not reflect the contribution of private hospitals and retail pharmacies to the consumption of antidiabetic drugs, even though this was a small proportion. Thirdly, due to the limitations of the data information, we were unable to analyse the relationship between market consumption and patient characteristics or prescriber information.
The study analysed the changing trends and use patterns of antidiabetic drugs and explored the impact of different pharmaceutical policies on drug use and expenditure. It was found that the use and expenditure of antidiabetic drugs showed a continuous upward trend in the last decade, and the prices of drugs were constantly reduced in the direction of benefiting the public, which was closely related to the increasing prevalence of the disease and the implementation of a series of pharmaceutical policies. The introduction of new antidiabetic drugs and changes in guideline recommendations have both influenced drug use patterns and led to significant increases in drug expenditure. This suggested that prevention of the disease is a key priority to reduce the financial burden on the health care system and individuals. In the future, the capacity of primary healthcare institutions to prevent and manage the disease should be improved as a whole, and the national basic public health service program should be carried out solidly, while at the same time strictly controlling the quality of the bid-winning drugs under the centralized purchasing policy, setting up an information system for the files of drug varieties, and steadily advancing the traceability management of the medicines that have been selected.
Availability of data and materials
The datasets generated or analysed during the current study are not publicly available due to confidentiality policies but are available from the corresponding author upon reasonable request.
Abbreviations
Centralised bidding and purchasing
Anatomical therapeutic chemistry
Defined daily dose
DDD per 1000 inhabitants per day
Defined daily cost
Essential medicines
World Health Organization
Gross domestic product
National Essential Medicine System
National Basic Medical Insurance Drug Catalogue
Dipeptidyl peptidase 4 inhibitors
Glucagon-like peptide-1 receptor analogue
Sodium-glucose co-transporter 2 inhibitors
Defined daily doses
Sun H, Saeedi P, Karuranga S, et al. IDF Diabetes Atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022;183:109119. https://doi.org/10.1016/j.diabres.2021.109119 .
Article PubMed Google Scholar
Li Y, Teng D, Shi X, et al. Prevalence of diabetes recorded in mainland China using 2018 diagnostic criteria from the American Diabetes Association: national cross sectional study. BMJ. 2020;369:m997. https://doi.org/10.1136/bmj.m997 .
Article PubMed PubMed Central Google Scholar
Xi T, Pan L, Ren X, et al. Analysis of the prevalence and influencing factors of prediabetes in Gansu Province. Chin J Dis Control. 2018;22(10):987–91. https://doi.org/10.16462/j.cnki.zhjbkz.2018.10.002 .
Article Google Scholar
Wang C, Hu Y, Hu X, et al. A study on accounting for diabetes treatment costs in Gansu Province based on the health cost accounting system 2011. Chronic Disease Prevention and Control in China. 2021;29(08):582-8. https://doi.org/10.16386/j.cjpccd.issn.1004-6194.2021.08.005 .
OECD. Health at a Glance. 2019. https://doi.org/10.1787/4dd50c09-en . Accessed 30 Jun 2023.
Book Google Scholar
Fang Y, Wagner AK, Yang S, et al. Access to affordable medicines after health reform: evidence from two cross-sectional surveys in Shaanxi Province, western China. Lancet Glob Health. 2013;1(4):e227-37. https://doi.org/10.1016/S2214-109X(13)70072-X .
Dong W, Zwi AB, Bai R, et al. Benefit of China’s social health insurance schemes: trend analysis and associated factors since health reform. Int J Environ Res Public Health. 2021;18(11):5672. https://doi.org/10.3390/ijerph18115672 .
Quan P, Hu X, Wang C, et al. Trends in hospitalization costs of diabetic patients in Gansu Province and analysis of factors affecting them, 2014–2018. Chronic Disease Prevention and Control in China. 2022;30(01):8–13. https://doi.org/10.16386/j.cjpccd.issn.1004-6194.2022.01.003 .
Shanghai Sunshine Pharmaceutical Purchasing Network. Notice on the announcement of the successful results of the centralized purchase of drugs in the union region. 2019. https://www.smpaa.cn/gjsdcg/2019/09/30/9040.shtml . Accessed 30 Jun 2023.
Google Scholar
Shanghai Sunshine Pharmaceutical Purchasing Network. Announcement of the proposed winning results of National Centralized Drug Purchasing. 2020. https://www.smpaa.cn/gjsdcg/2020/01/17/9261.shtml . Accessed 30 Jun 2023.
Shanghai Sunshine Pharmaceutical Purchasing Network. Notice on the announcement of the winning results of the National Centralized Purchasing of Pharmaceuticals. 2020. https://www.smpaa.cn/gjsdcg/2020/08/24/9560.shtml . Accessed 30 Jun 2023.
Lanzhou Municipal Bureau of Medical Protection. Supply list of selected drugs in the fourth batch of National Collective Purchasing (Gansu). 2021. http://ybj.lanzhou.gov.cn/art/2021/7/22/art_15304_1030279.html . Accessed 30 Jun 2023.
Lanzhou Municipal Bureau of Medical Protection. Supply list of selected medicines in Gansu Province collective purchasing (Fifth Batch 2021.10.15-2022.10.14). 2021. http://ybj.lanzhou.gov.cn/art/2022/4/27/art_15304_1114981.html . Accessed 30 Jun 2023.
CHINANEWS. Gansu to reduce the burden of public medicine: the collection of drug cost savings of more than 1.3 billion yuan. 2021. https://www.chinanews.com.cn/cj/2021/07-27/9529748.shtml . Accessed 30 Jun 2023.
Bucsa C, Farcas A, Iaru I, Mogosan C, Rusu A. Drug utilisation study of antidiabetic medication during 2012–2019 in Romania. Int J Clin Practice. 2021;75(11):e14770. https://doi.org/10.1111/ijcp.14770 .
Article CAS Google Scholar
Moura AM, Martins SO, Raposo JF. Consumption of antidiabetic medicines in Portugal: results of a temporal data analysis of a thirteen-year study (2005–2017). BMC Endocrine Disorders. 2021;21(1):1–10. https://doi.org/10.1186/s12902-021-00686-w .
National Bureau of Statistics of China. China statistics yearbook. 2021. http://www.stats.gov.cn/sj/ndsj/2022/indexch.htm . Accessed 30 Jun 2023.
Dang Y, Yang Y, Yang A, et al. Factors influencing catastrophic health expenditure of households with people with diabetes in Northwest China-an example from Gansu Province. BMC Health Serv Res. 2023;23(1):401. https://doi.org/10.1186/s12913-023-09411-w .
Gansu Taxation Bureau of the State Administration of Taxation. Gansu daily: let the people feel more livelihood temperature. 2021. http://gansu.chinatax.gov.cn/art/2021/3/17/art_289_245484.html . Accessed 30 Jun 2023.
Csatordai M, Benko R, Matuz M, et al. Use of glucose-lowering drugs in Hungary between 2008 and 2017: the increasing use of novel glucose-lowering drug groups. Diabet Med. 2019;36(12):1612–20. https://doi.org/10.1111/dme.14117 .
Article CAS PubMed Google Scholar
The WHO Collaborating Centre for Drug Statistics Methodology. Implementation and maintenance of the ATC/DDD methodology. 2022. https://www.whocc.no/use_of_atc_ddd/ . Accessed 30 Jun 2023.
Gansu Provincial Bureau of Statistics. Gansu Province statistics yearbook. 2021. http://tjj.gansu.gov.cn/tjj/c109464/info_disp.shtml . Accessed 30 Jun 2023.
National Health Commission Floating Population Service Center. Data from China floating population dynamic monitoring survey. 2021. https://www.chinaldrk.org.cn/wjw/#/data/classify/population/provinceList . Accessed 30 Jun 2023.
CEIC statistical database. Gansu, China: Consumer Price Index. 2021. https://www.ceicdata.com/zh-hans . Accessed 30 Jun 2023.
Reed J, Bain S, Kanamarlapudi V. A review of current trends with type 2 diabetes epidemiology, aetiology, pathogenesis, treatments and future perspectives. Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy. 2021;14:3567–602. https://doi.org/10.2147/DMSO.S319895 .
Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes, 2015: a patient-centered approach: update to a position statement of the American Diabetes Association and the European Association for the study of diabetes. Diabetes Care. 2015;38(1):140–9. https://doi.org/10.2337/diaspect.25.3.154 .
Khawandanah J. Double or hybrid diabetes: a systematic review on disease prevalence, characteristics and risk factors. Nutr Diabetes. 2019;9(1):33. https://doi.org/10.1038/s41387-019-0101-1 .
Bang C, Mortensen MB, Lauridsen KG, Bruun JM. Trends in antidiabetic drug utilization and expenditure in Denmark: A 22-year nationwide study. Diabetes Obes Metab. 2020;22(2):167–72. https://doi.org/10.1111/dom.13877 .
Fürnsinn C, Śliwczyński A, Brzozowska M, et al. Drug-class-specific changes in the volume and cost of antidiabetic medications in Poland between 2012 and 2015. Plos One. 2017;12(6):e0178764. https://doi.org/10.1371/journal.pone.0178764 .
Dang Y, Yang Y, Cao S, et al. Exploring the factors influencing the use of health services by people with diabetes in Northwest China: an example from Gansu Province. J Health Popul Nutr. 2023;42(1):64. https://doi.org/10.1186/s41043-023-00402-5 .
People's Daily Online (PRC newspaper). Gansu Province, a number of health insurance policies to benefit the people to be implemented from next year. 2022. http://gs.people.com.cn/n2/2022/1209/c183283-40224921.html . Accessed 30 Jun 2023.
Harsch IA, Kaestner RH, Konturek PC. Hypoglycemic side effects of sulfonylureas and repaglinide in ageing patients - knowledge and self-management. J Physiol Pharmacol. 2018;69(4). https://doi.org/10.26402/jpp.2018.4.15 .
Fang M, Wang D, Coresh J, et al. Trends in diabetes treatment and control in U.S. adults, 1999–2018. N Engl J Med. 2021;384(23):2219–28. https://doi.org/10.1056/NEJMsa2032271 .
Chen Y, Li Q, Han Y, et al. Vildagliptin versus alpha-glucosidase inhibitor as add-on to metformin for type 2 diabetes: subgroup analysis of the China Prospective Diabetes Study. Diabetes Ther. 2020;11(1):247–57. https://doi.org/10.1007/s13300-019-00742-8 .
Alssema M, Ruijgrok C, Blaak EE, et al. Effects of alpha-glucosidase-inhibiting drugs on acute postprandial glucose and insulin responses: a systematic review and meta-analysis. Nutr Diabetes. 2021;11(1):11. https://doi.org/10.1038/s41387-021-00152-5 .
Article CAS PubMed PubMed Central Google Scholar
Ministry of Human Resources and Social Security of China. Circular of the Ministry of Human Resources and Social Security on printing and issuing the drug catalogue of National Basic Medical Insurance, Industrial Injury Insurance and Maternity Insurance (2017 Edition). 2017. http://www.mohrss.gov.cn/SYrlzyhshbzb/shehuibaozhang/zcwj/yiliao/201702/t20170223_266775.html . Accessed 30 Jun 2023.
Gregg EW, Sattar N, Ali MK. The changing face of diabetes complications. Lancet Diabetes Endocrinol. 2016;4(6):537–47. https://doi.org/10.1016/S2213-8587(16)30010-9 .
Sun X, Meng H, Ye Z, et al. Factors associated with the choice of primary care facilities for initial treatment among rural and urban residents in Southwestern China. PLoS One. 2019;14(2):e0211984. https://doi.org/10.1371/journal.pone.0211984 .
Liu Y, Zhong L, Yuan S, et al. Why patients prefer high-level healthcare facilities: a qualitative study using focus groups in rural and urban China. BMJ Glob Health. 2018;3(5):e000854. https://doi.org/10.1136/bmjgh-2018-000854 .
Vaughan EM, Rueda JJ, Samson SL, et al. Reducing the burden of diabetes treatment: a review of low-cost oral hypoglycemic medications. Curr Diabetes Rev. 2020;16(8):851–8. https://doi.org/10.2174/1573399816666200206112318 .
Yao Q, Liu C, Ferrier JA, Liu Z, Sun J. Urban-rural inequality regarding drug prescriptions in primary care facilities – a pre-post comparison of the National Essential Medicines Scheme of China. Int J Equity Health. 2015;14(1):1–9. https://doi.org/10.1186/s12939-015-0186-7 .
Dong Z, Tao Q, Sun G. Survey and analysis of the availability and affordability of essential drugs in Hefei based on WHO / HAI standard survey methods. BMC Public Health. 2020;20(1):1405. https://doi.org/10.1186/s12889-020-09477-9 .
Liu GG, Vortherms SA, Hong X. China’s health reform update. Annu Rev Public Health. 2017;38:431–48. https://doi.org/10.1146/annurev-publhealth-031816-044247 .
Sun J, Lyu S. The effect of medical insurance on catastrophic health expenditure: evidence from China. Cost Effectiveness and Resource Allocation. 2020;18(1):1–11. https://doi.org/10.1186/s12962-020-00206-y .
Yu X, Mao N. Analysis of the causes of abnormal fluctuations in drug prices and proposals for countermeasures. Health Economics Research. 2021;38(7):44–7 ( https://kns.cnki.net/kcms/detail/33.1056.F.20210701.1746.020.html ).
State Council of the People’s Republic of China. Pilot program for national centralized drug procurement and use. 2019. http://www.gov.cn/zhengce/content/2019-01/17/content_5358604.htm . Accessed 30 Jun 2023.
Yang Y, Tong R, Yin S, et al. The impact of “4 + 7” volume-based drug procurement on the volume, expenditures, and daily costs of antihypertensive drugs in Shenzhen, China: an interrupted time series analysis. BMC Health Serv Res. 2021;21(1):1275. https://doi.org/10.1186/s12913-021-07143-3 .
Yang Y, Chen L, Ke X, et al. The impacts of Chinese drug volume-based procurement policy on the use of policy-related antibiotic drugs in Shenzhen, 2018–2019: an interrupted time-series analysis. BMC Health Serv Res. 2021;21(1):668. https://doi.org/10.1186/s12913-021-06698-5 .
Download references
Acknowledgements
We thank the Special Research on Lanzhou University Serving Gansu Economic and Social Development (contract number 2019-FWZX-11) and Research on Total Health Expenditure in Gansu Province (contract number 2022620005002671) for supporting this study.
This study was supported by Special Research on Lanzhou University Serving Gansu Economic and Social Development (contract number 2019-FWZX-11) and Research on Total Health Expenditure in Gansu Province (contract number 2022620005002671).
Author information
Authors and affiliations.
School of Public Health, Lanzhou University, 222# Tianshui South Road, Lanzhou, 730000, China
Wenxuan Cao, Hu Feng, Yaya Yang, Lei Wang, Xuemei Wang & Xiaobin Hu
Division of Pharmaceutical Procurement, Gansu Public Resources Trading Center, 68# Yanxing Road, Lanzhou, 730000, China
Yongheng Ma & Defang Zhao
You can also search for this author in PubMed Google Scholar
Contributions
Yongheng Ma and Defang Zhao provided data and technical support, Hu Feng and Yaya Yang carried out partial data management, Lei Wang and Xuemei Wang polished the language, Xiaobin Hu provided critical comments, and Wenxuan Cao analyzed the data and wrote the manuscript. All authors read and approved the final manuscript.
Corresponding author
Correspondence to Xiaobin Hu .
Ethics declarations
Ethics approval and consent to participate.
Not applicable. No ethical approval was required for this study by the author’s institution because this research only included the medication procurement information and all the information was anonymous. No secondary data were used in this study and no humans were involved.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Cao, W., Feng, H., Yang, Y. et al. Trends in antidiabetic drug use and expenditure in public hospitals in Northwest China, 2012-21: a case study of Gansu Province. BMC Health Serv Res 24 , 415 (2024). https://doi.org/10.1186/s12913-024-10917-0
Download citation
Received : 16 August 2023
Accepted : 27 March 2024
Published : 03 April 2024
DOI : https://doi.org/10.1186/s12913-024-10917-0
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Antidiabetic drug
- Public hospitals
- Use pattern
- Pharmaceutical policy
BMC Health Services Research
ISSN: 1472-6963
- General enquiries: [email protected]
HPE MyAccount
Your HPE MyAccount provides you with:
- Single sign-on to the HPE ecosystem
- Personalized recommendations
- Test drives and other trials
- And many more exclusive benefits
HPE Ecosystem
Hpe greenlake.
- Cloud Consoles
- Cloud Services
- Data Services
- Compute Ops Management
- Aruba Central
- HPE GreenLake Administration
- Manage Account
- Manage Devices
- HPE Resources
- Support Center
- Financial Services
- Communities
Your open and secure edge-to-cloud platform that powers data-first modernization
Control and harness data across edge to cloud.
A single source of truth from data to make smart decisions and recommendations to customers.
Create your AI advantage by unlocking the full potential of your data.
Hybrid cloud, just the way you need it.
Only the right level of security will do.
- Product types
- Solutions by topic
Accelerate your data-first modernization with the HPE GreenLake edge-to-cloud platform, which brings the cloud to wherever your apps and data live.
- Supercomputing
- HPE Cray Supercomputing
- HPE ProLiant Compute
- HPE Alletra Storage
- HPE Aruba Networking
- HPE Ezmeral Software
- HPE Services
- HPE GreenLake for Networking
- HPE GreenLake for Block Storage
- HPE GreenLake for Private Cloud Enterprise
- HPE GreenLake for Compute Ops Management
- HPE GreenLake for Disaster Recovery
- HPE GreenLake for Backup and Recovery
- Learn about HPE
- Corporate social responsibility
- HPE education services
- Certification and learning
- FREE on-demand developer workshops
- FREE on-demand technical courses
- Customer success stories
- Reference architectures
- Quick specs
- What is edge to cloud?
- HPE GreenLake FAQ
- HPE GreenLake Central user guide
HPE SimpliVity
Step into the future with an intelligent, hyper-efficient HCI solution that’s optimized for your edge, VDI, and general virtualization workloads.
We've reimagined what your HCI can be
Picture a hyperconverged architecture that’s evolved beyond software-defined to AI-driven — and delivers self-managing, self-optimizing, and self-healing infrastructure. By adding the machine learning predictive analytics of HPE InfoSight to our hyperconverged platform, we’ve ushered in the era of intelligent HCI.
cost savings Forrester%20Total%20Economic%20Impact%20of%20HPE%20SimpliVity%20report
vs. traditional infrastructure
data efficiency, guaranteed %3Ca%20href%3D%22https%3A%2F%2Fwww.hpe.com%2Fus%2Fen%2Fproducts%2Fintegrated-systems%2Fsimplivity-guarantee.html%22%20data-analytics-region-id%3D%22footnote_tip%7Clink_click%22%3EHPE%20SimpliVity%20HyperGuarantee%3C%2Fa%3E
across storage and backup
specialists required
enjoy a simple consumer experience
Not your ordinary HCI
With simplicity that’s powered by HPE InfoSight, the most advanced AI for infrastructure, HPE SimpliVity is ideal for edge, ROBO, VDI, and general virtualization use cases. VM-centric management and mobility, built-in backup and DR, and game-changing data efficiency combine in a hyperconverged architecture that’s optimized from data center to edge.
Drive app modernization with containers
Accelerate your adoption of agile, cloud-native, containerized apps. With HPE SimpliVity, there’s no need for separate systems to power VMs and containers: the Container Storage Interface (CSI) Driver for Kubernetes enables you to easily run everything on a single platform — without additional infrastructure.
Get the most efficient, all-in-one HCI
Take advantage of HPE SimpliVity’s unrivaled efficiency — with HA across just two nodes and enterprise-grade data services and security built-in.
Consume HPE SimpliVity on demand
Leverage the flexibility and ease of use of industry-leading hyperconverged — but in a consumption-based model that delivers exactly the IT you need, when you need it. HPE SimpliVity is now available as a service through HPE GreenLake.
Enable intelligently simple management
Accelerate time to market and bring an end to IT fire-fighting. Software-defined automation simplifies and speeds day 0 and 1, while artificial intelligence predicts and prevents problems to optimize day 2 and beyond.
Enjoy 90% capacity savings, guaranteed
The hyper efficiency baked into HPE SimpliVity improves application performance, frees up storage, and accelerates local and remote backup and restore functions. We guarantee a 90% capacity savings across storage and backup combined — and you enjoy 10:1 data efficiency.
Remain online and recoverable — always
Leverage built-in backup and disaster recovery to ensure business continuity. HPE SimpliVity’s speed and efficiency enable recovery of a 1 TB VM in 60 seconds. Now you can deploy and consolidate workloads on HPE SimpliVity.
Drive savings for edge and ROBO workloads
HPE SimpliVity’s efficient data services, centralized management, and comprehensive data protection and disaster recovery deliver savings of up to 66% versus traditional three-tier, cloud, or other HCI infrastructure.
Our customers
TSPL chose the HPE hyperconverged infrastructure to revamp and streamline its IT operations by consolidating its legacy server and storage environment.
Federation University Australia
Federation University Australia transforms the efficiency and agility of its IT infrastructure to accelerate digital innovation for 25,000 students across four campuses.
Fino Payments Bank
Fino Payments Bank is set to transform the lives of India’s rural population and power the country’s next great economic leap with smart, efficient IT infrastructure management.
Unichem Laboratories Ltd.
Unichem Laboratories Ltd. is lowering the cost and extending the availability of life-saving treatments by accelerating discovery, development, and production.
Chase Center
The Golden State Warriors built Chase Center to exceed fan expectations with a technology foundation that enables choice, control, and safety. Chase Center is a new breed of venue.
Power and protect your virtualized infrastructure
Simplify the VM experience by delivering true hyperconvergence at scale — from edge to data center — with efficiency, resiliency, density, and simplicity.
Reduce capacity requirements with operational efficiency
Operational efficiency reduces capacity requirements and improves application speed and performance. Always-on, inline deduplication and compression only needs to happen once, delivering 90% capacity savings across primary storage and backup – guaranteed! Key features include:
- Data efficiency - Always-on, at inception, inline deduplication and compression guarantees 90% capacity savings across primary storage and backup saving costs
- Application performance - Achieve improved performance from all-flash storage, tiered caching, and always-on, inline dedupe and compression
- Operational efficiency - Operational efficiency frees up 91% of IT organizations’ time to focus on new projects
Achieve resiliency and high availability
Achieve high availability with just 2 nodes. HPE SimpliVity tolerates simultaneous drive failures without data loss, and built-in data protection and disaster recovery features help keep data safe. Key features include:
- High availability - High availability tolerates simultaneous drive failures without data loss and achieves high availability with a minimum of 2 nodes
- Backup - Full logical VM backups with policy-based automation and near zero overhead
- Restore - Guaranteed 60-second restore of 1 TB VM
- Disaster recovery - Automated, multi-site, rapid disaster recovery reduces the risk of data loss and costly business downtime
Leverage high-density resource pools
Flexible, consolidated resource pools are cost effective building blocks for a variety of workloads. The award-winning HPE SimpliVity 2600 provides space-constrained environments with high-density, enterprise grade features and functionality. Key features include:
- Collapse the stack into one solution - Flexible resource pools of compute, storage, and composable fabric networking collapsed into one solution
- Scale - Simple, parallel node deployment to scale out from small to large VM environments in small, 2U increments
- Consolidation and cost savings - Simplify and save: one solution, one refresh cycle, one generalist needed to manage the whole stack
Simplify management with a single interface
Simple and automated operations eliminate the need for specialized IT skills. VM administrators manage the entire IT stack from a single, familiar interface. Back up, clone, or restore a VM in 3 clicks, guaranteed, using policy-based, VM-centric management. Key features include:
- VM-centric management - Policy-based, global VM-centric management with automation, visibility, intelligence
- VM agility - VM creation, backup, replication, and recovery with right-click operations from familiar interface
- VM mobility - Moves VMs quickly and globally from one site to another
- Simple management from one interface - No LUNS, shares, or volumes to manage. Through a single interface, you have a global view into data centers as well as remote and branch offices
HPE a Gartner Magic Quadrant Leader 14 years in a row
Gartner® again names HPE a Leader in the 2023 Magic Quadrant™ for Primary Storage.
Hyperconverged technology partners
Explore the hpe simplivity portfolio.
HPE SimpliVity 380 gives IT organizations the agility and economics of the cloud with the control and governance of on-premises IT and HPE GreenLake for Private Cloud Business Edition integration. It delivers a powerhouse hyperconverged solution optimized to support the world’s most efficient and resilient data centers. This solution dramatically simplifies IT by combining infrastructure and advanced data services for virtualized workloads on a single device.
Do you need a dense platform with built-in security and flexibility that addresses key applications which need performance, availability along with ease of management? HPE SimpliVity 325 provides HCI choice with our 3rd Generation AMD EPYC™ single CPU processor platform including all-flash storage. Highly dense, the solution is a 1U enclosure that scales in 1U increments and is ideal for remote office or space-constrained locations.
Featured products
Hpe storeonce backup appliances.
Secure your data wherever it lives. Leverage intelligent storage to transform your hybrid cloud data protection with greater simplicity, higher performance, and built-in ransomware protection — all at a lower cost than traditional solutions.
HPE GreenLake for Virtual Desktop Infrastructure
Empower your remote workforce with secure, scalable virtual desktop infrastructure, delivered as a service.
HPE Alletra dHCI
Built to streamline your infrastructure via data-first modernization, HPE’s disaggregated HCI for mixed workloads at scale unlocks IT agility while ensuring apps are always-on and always-fast.
Adopting hyperconvergence and adapting to the new realities in retail
Accelerate your data-driven transformation with simplivity, hpe simplivity 380 product documentation, technical specifications, advanced data services.
- Built-in resiliency, backup, and disaster recovery for data protection
- Always-on deduplication and compression for reduced capacity utilization by up to 10X — guaranteed %3Ca%20href%3D%22https%3A%2F%2Fwww.hpe.com%2Fus%2Fen%2Fproducts%2Fintegrated-systems%2Fsimplivity-guarantee.html%22%20data-analytics-region-id%3D%22footnote_tip%7Clink_click%22%3EHPE%20SimpliVity%20HyperGuarantee%3C%2Fa%3E
Flexible federation strategy
- Scale up to 16 nodes/cluster and 96 nodes/federation
- Mix clusters within the same federation — for example, HPE SimpliVity 380 at the core data center and HPE SimpliVity 325 or 380 at the edge
Simple, intelligent management
- Global, VM-centric management and mobility, plus artificial intelligence by HPE InfoSight
Simplify your environment with HPE SimpliVity 380
- Storage-intensive workloads
- Multiple all-flash configuration options (XS, S, M, L, and XL)
- Backup and archive node with hybrid flash storage
- Hardware-accelerated or software-optimized for always-on deduplication and compression
Extend your options with HPE SimpliVity 325
- Small ROBO and edge use cases
- Highly dense, 1U, single AMD processor node with high core count
- Full HPE SimpliVity functionality
Optimize your data center footprint with HPE SimpliVity 325
- General purpose virtualization, edge, and VDI workloads
- Space-constrained environments that need a high-density server form factor
- Software-optimized for always-on deduplication and compression
Facilitators and barriers in the use of the electronic consultation register for Integrated Management of Childhood Illness in the health district of Toma, Burkina Faso: Perspectives of health care providers
- Find this author on Google Scholar
- Find this author on PubMed
- Search for this author on this site
- ORCID record for Ngangue Patrice
- For correspondence: [email protected]
- Info/History
- Preview PDF
Background In collaboration with the Ministry of Health and Public Hygiene (MHPH) of Burkina Faso (BF), the Foundation Terre des Hommes (Tdh) has developed the Integrated e-Diagnostic Approach (IeDA) project in BF since 2010 to strengthen the health system by digitalizing medical protocols, improving the quality of services and using data. We sought to identify and analyze the barriers and facilitators of using the electronic clinic registry (ECR) for the integrated management of childhood illness (IMCI) by healthcare providers (HCPs) in the health district of Toma, BF.
Methods We conducted a descriptive and exploratory qualitative study. In-depth individual interviews were conducted with thirty-five (35) HCPs in the health district of Toma, BF, from the 1 st to the 30 th of December 2021. Thematic analysis of qualitative data according to the Braun & Clarke model was performed using NVivo 12 software and arranged along a social-ecological model.
Results Our findings revealed that HCPs play an essential role in using ECR for IMCI. Many key facilitating factors have emerged regarding the use of IMCIs in primary health care (PHC) facilities, such as positive perceptions of the ECR, firm commitment and the involvement of HCPs, stakeholder support, collaborative networks with implementing partners, convenience, privacy, confidentiality and client trust, experience and confidence in using the system, and the satisfaction, motivation and competency of staff. In addition, the easy diagnosis offered by the ECR and the training of HCPs increased the acceptance and use of the ECR. Regarding barriers, HCPs complained about the tablet’s slowness, recurrent breakdowns, and increased workload.
Conclusion This study revealed that ECR has excellent potential to improve the quality of care and, in turn, reduce maternal and infant mortality. Although the satisfaction of the HCPs with the tool is positive, the actors of the Foundation Tdh, in collaboration with the MHPH, must work to optimize the application’s performance and reduce breakdowns and delays during consultations. This will allow the deployment of ECR in all BF health districts.
Competing Interest Statement
The authors have declared no competing interest.
Funding Statement
This study did not receive any funding
Author Declarations
I confirm all relevant ethical guidelines have been followed, and any necessary IRB and/or ethics committee approvals have been obtained.
The details of the IRB/oversight body that provided approval or exemption for the research described are given below:
The study received approval from the Burkina Faso Health Research Ethics Committee under deliberation number 2021-12-283. Investigation authorization was also obtained from the chief physician of the health district of Toma. Furthermore, the patients/participants provided written informed consent to participate in this study.
I confirm that all necessary patient/participant consent has been obtained and the appropriate institutional forms have been archived, and that any patient/participant/sample identifiers included were not known to anyone (e.g., hospital staff, patients or participants themselves) outside the research group so cannot be used to identify individuals.
I understand that all clinical trials and any other prospective interventional studies must be registered with an ICMJE-approved registry, such as ClinicalTrials.gov. I confirm that any such study reported in the manuscript has been registered and the trial registration ID is provided (note: if posting a prospective study registered retrospectively, please provide a statement in the trial ID field explaining why the study was not registered in advance).
I have followed all appropriate research reporting guidelines, such as any relevant EQUATOR Network research reporting checklist(s) and other pertinent material, if applicable.
Data Availability
All data produced in the present work are contained in the manuscript
View the discussion thread.
Thank you for your interest in spreading the word about medRxiv.
NOTE: Your email address is requested solely to identify you as the sender of this article.

Citation Manager Formats
- EndNote (tagged)
- EndNote 8 (xml)
- RefWorks Tagged
- Ref Manager
- Tweet Widget
- Facebook Like
- Google Plus One
Subject Area
- Primary Care Research
- Addiction Medicine (316)
- Allergy and Immunology (618)
- Anesthesia (160)
- Cardiovascular Medicine (2277)
- Dentistry and Oral Medicine (279)
- Dermatology (201)
- Emergency Medicine (370)
- Endocrinology (including Diabetes Mellitus and Metabolic Disease) (798)
- Epidemiology (11579)
- Forensic Medicine (10)
- Gastroenterology (678)
- Genetic and Genomic Medicine (3582)
- Geriatric Medicine (336)
- Health Economics (617)
- Health Informatics (2305)
- Health Policy (913)
- Health Systems and Quality Improvement (864)
- Hematology (335)
- HIV/AIDS (753)
- Infectious Diseases (except HIV/AIDS) (13154)
- Intensive Care and Critical Care Medicine (757)
- Medical Education (359)
- Medical Ethics (100)
- Nephrology (389)
- Neurology (3351)
- Nursing (191)
- Nutrition (507)
- Obstetrics and Gynecology (651)
- Occupational and Environmental Health (646)
- Oncology (1758)
- Ophthalmology (525)
- Orthopedics (209)
- Otolaryngology (284)
- Pain Medicine (223)
- Palliative Medicine (66)
- Pathology (438)
- Pediatrics (1004)
- Pharmacology and Therapeutics (422)
- Primary Care Research (406)
- Psychiatry and Clinical Psychology (3062)
- Public and Global Health (5992)
- Radiology and Imaging (1223)
- Rehabilitation Medicine and Physical Therapy (715)
- Respiratory Medicine (811)
- Rheumatology (367)
- Sexual and Reproductive Health (353)
- Sports Medicine (316)
- Surgery (386)
- Toxicology (50)
- Transplantation (170)
- Urology (142)
Biden to discuss new student loan forgiveness plan in Wisconsin on Monday: Sources
The White House would not yet confirm any details.
President Joe Biden is expected to discuss the framework for a new major student loan forgiveness plan on Monday during a trip to Wisconsin, sources familiar with the White House's plans confirm to ABC News.
Biden is scheduled to travel on Monday to Madison, home to a major university and in a crucial battleground state.

A proposed rule that could impact millions of borrowers may be close to being finalized, sources said. The White House would not yet confirm any details.
The latest proposal was first reported by The Wall Street Journal on Friday.
MORE: Biden administration begins canceling student loan debt for 804,000 borrowers
Sources told ABC News that unlike the sweeping student loan forgiveness plan that was struck down by the Supreme Court last year, this new one will require borrowers to fall into specific categories to get relief, such as possible financial hardship or holding debt that because of interest is now bigger than the amount originally borrowed.
That distinction -- a more targeted approach to debt cancellation -- is part of what makes the White House confident in their legal footing this time should a new proposal be challenged as well, sources said.
Related Stories

President Joe Biden will unveil his new plan to give student loan relief to many new borrowers
- Apr 5, 11:47 AM

An appeals court blocks a debt relief plan for students who say they were misled by colleges
- Apr 5, 6:05 PM

New US-China talks will address a top American complaint about Beijing's economic model, Yellen says
- Apr 5, 11:27 PM
The Department of Education has been engaged in recent months in public listening sessions with stakeholders -- a move considered best practice and a way to firm up justification and standing for new regulations.
MORE: Biden administration forgives student loans for 78,000 more public service workers
The Supreme Court struck down the Biden administration's initial loan forgiveness plan in June 2023. In a 6-3 decision, the court ruled the Department of Education exceeded its authority when it moved to wipe out more than $400 billion in federal student loan debt.
The program would have forgiven up to $10,000 in debt for borrowers making less than $125,000 a year. Borrowers who took out Pell Grants to pay for college could have had up to $20,000 canceled.
Forty-three million Americans would have qualified for the program, and the Education Department had already approved applications for 16 million borrowers before halting due to legal challenges.
Biden, who made tackling student loan debt a key campaign pledge, said following the ruling that "the fight is not over."
Related Topics
- President Biden
Wisconsin doctor who sued to protect abortion access joins congressional race
- Apr 4, 11:37 AM

Republican states file lawsuit challenging Biden's student loan repayment plan
- Mar 28, 3:18 PM
ABC News Live
24/7 coverage of breaking news and live events
IMAGES
VIDEO
COMMENTS
The Partnership for Public Service, a think-tank, suggests that more than 80 different federal occupations are likely to be affected by automation (Partnership for Public Service, 2019[4]). With a recent study suggesting that 60% of all new hires leave the US Federal workforce after less than two years, preventing skills gaps is a key priority ...
The strategy paid off. In 2017, Patel launched an ambitious public-private private partnership—the Kidney Innovation Accelerator, or KidneyX—that redefined how the federal government tackles kidney disease. The initiative began as a "moonshot approach to developing alternatives to dialysis.". According to Patel, it's goal was to ...
This report is a collation of the select examples and case studies undertaken in different countries as part of their respective public service delivery reform agenda. Each country provides a unique learning for improvement of public service delivery in Albania. As part of the Best Practices study, the following five countries have been considered.
Francis Collins: A commitment to public good, public health and public service leadership. In the 1980s, a young scientist at the University of Michigan was working to identify the gene that causes cystic fibrosis, an inherited disease that researchers had been investigating for years. Hitting roadblock after roadblock, the scientist was faced ...
The SDGs ultimately aim to end poverty, protect the planet, and provide a prosperous future for all. The case studies feature 17 different countries, detailing the progress made in each of the 17 SDGs (one Goal per country). In doing so, the cases illustrate the critical role the public sector played in making progress on the SDG in each country.
Although New Public Service (NPS) principles are well known, their practice in local government settings has only been limitedly explored. As a means of better understanding governance practices that adhere to NPS principles in local contexts, this study engaged in a case study of Grand Island, New York.
Public Service: State of Transformation. 2018 case studies from the Public Service Transformation Academy. First published 2018 by Public Service Transformation Publishing. 27-29 South Lambeth Road London SW8 1SZ [email protected] 0203 771 2608. ISBN. 978-1-9996851-1-9 (self-printed) 978-1-9996851-3-3 (electronic version)
Analysing two different case studies, this study reflects on the tenability of Huberts' value panorama of seven central governance values and will examine this position for two different types of public contexts. These two case studies will put values in context along the lines of two specific administrative types of public service delivery ...
This study explores confidence levels in the public service in Alberta amid the COVID-19 pandemic, using data from the April 2022 Viewpoint Alberta survey. Our findings illuminate diverse attitudes towards public servants amidst significant social, economic, and political upheaval. ... Using Alberta as a case study, we examine the levels of ...
This edition presents a vision of a future-ready public service workforce that is forward-looking, flexible and fulfilling to a diverse range of public employees. It provides insights to help governments achieve that vision through comparative data and analysis, a set of illustrative case studies, and expert commentary.
Case Studies in Public Services Management examines key issues such as managing networks, measuring performance, changing culture, implementing strategy and strategic change. In addressing the key contemporary issues in public services management the cases cover a range of functions including education, health, community care, welfare benefits and policing.
They can test theories in multiple ways and create or suggest new theories. Considering field-level questions as a case study and synthesizing findings from multiple related studies, regardless of methodology, can help move the field forward in terms of its connection between theory and practice, art and science.
Governments are altering how they operate to enhance the provision of public services, be more successful and efficient in their plans, and accomplish goals such as greater transparency, interoperability, and citizen pleasure. There are, however, limited studies about how public sector managers are currently identifying digital transformation in their own day-to-day practices, how they are ...
THE THIRD SECTOR, USER INVOLVEMENT AND PUBLIC SERVICE REFORM: A CASE STUDY IN THE CO-GOVERNANCE OF HEALTH SERVICE PROVISION. GRAHAM P. MARTIN, GRAHAM P. MARTIN. Graham P. Martin is in the Department of Health Sciences, University of Leicester. Search for more papers by this author.
Stewardship of Public Trust. Given the vast influence, power and resources of our government, trust in federal leaders and their integrity is paramount. Federal leaders represent the public and must be held to the highest standards. They are stewards of the Constitution, taxpayer dollars and the workforces they lead. Read the stewardship case study
The effect of leadership on public service motivation: a multiple embedded case study in Morocco. Zakaria Belrhiti, 1, 2, 3 Wim Van Damme, 2, 3 Abdelmounim Belalia, 1 and Bruno Marchal 2 ... We adopted a multiple case study design 107 because it fits the exploration of multifaceted complex phenomena, such as PSM, in real-world settings (in our ...
Two cases about Hertz claimed top spots in 2021's Top 40 Most Popular Case Studies. ... Master's in Public Education Management One-year program for leaders in urban public school systems. ... IBM Corporate Service Corps. 21. Business Leadership in South Africa's 1994 Reforms. 22. Alternative Meat Industry.
Abstract. This study aimed at identifying the implementation of bureaucratic reforms and trying to offer some solutions for improvement of administrative services licensing. This study applied ...
The public sector group was struggling to maintain productivity with its existing legacy investment, and felt a dire need to upgrade to a new solution capable of serving 53 offices across 30 global locations. Fortunately, switching to Zoom allowed the organisation to leverage a new, more efficient mode of communication for its modern workforce.
ABSTRACT. Although it is generally acknowledged that the raison d'être for public service media (PSM) is to serve the public, there is much less agreement about what the term specifically means. This contribution, using a recent newsroom conflict at the Slovak public service broadcaster Radio and Television of Slovakia (RTVS) as a case study, explores how PSM journalists and managers perceive ...
The paper undertakes four in-depth country case studies and the public management reforms as a response to institutional pressure are examined using the 4M strategy (Pollitt and Bouckaert, 2017)-Maintain (holding on to existing administrative structures and processes), Modernize (keeping service delivery and regulation up to date), Marketize ...
Abstract. This study aims to examine and analyze how the ethics of bureaucrats in public service in the field of land, and detect factors that affect the ethics of public service bureaucrats in the field of land, as well as find effective solutions for the apparatus in enforcing the ethics of public services in accordance with the established moral standards and standard rules.
Introduction. The ubiquitous collection and use of digital data is changing people's lives, positively and negatively. Many commentators believe that it is vital that public views are factored into decisions that will shape the future of the data economy, and this has led to increasing interest in how the public perceives 'data practices' (that is, organisations collecting, analysing and ...
An AT&T store in New York. The telecommunications company said Saturday that a data breach has compromised the information tied to 7.6 million current customers. AT&T announced on Saturday it is ...
Overview of the use of antidiabetic drugs. During the ten-year study period, the overall trend of antidiabetic drug use and expenditure in Gansu Province was increasing (B = 1.373, 44.229, P < 0.001), use increased from 1.04 in 2012 to 16.02 DID in 2021, and expenditure increased from 48.36 in 2012 to 496.42 million yuan in 2021 (from 7.66 to 76.95 million USD), with the largest increase in ...
HPE SimpliVity. 380 series. HPE SimpliVity 380 gives IT organizations the agility and economics of the cloud with the control and governance of on-premises IT and HPE GreenLake for Private Cloud Business Edition integration. It delivers a powerhouse hyperconverged solution optimized to support the world's most efficient and resilient data ...
Background In collaboration with the Ministry of Health and Public Hygiene (MHPH) of Burkina Faso (BF), the Foundation Terre des Hommes (Tdh) has developed the Integrated e-Diagnostic Approach (IeDA) project in BF since 2010 to strengthen the health system by digitalizing medical protocols, improving the quality of services and using data. We sought to identify and analyze the barriers and ...
Litigation attorney Kristin Asai was mentioned in an article published by Oregon Public Broadcasting (OPB) about a case before the Oregon Supreme Court on whether judges can force public defenders to take new clients.The case arose when judges in Marion County forced a public defender at a nonprofit firm to take a new client, despite objections that taking on more clients than an attorney can ...
The Supreme Court struck down the Biden administration's initial loan forgiveness plan in June 2023. In a 6-3 decision, the court ruled the Department of Education exceeded its authority when it ...
Federal authorities are downplaying the public health risk after the second ever case of a human contracting the "highly pathogenic" bird flu in the United States was confirmed in Texas on Monday.